Usc Chart Review Worksheet Sample
ADVERTISEMENT
 1
1 2
2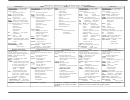 3
3USC Chart Review Worksheet Sample
Claim Adjustment? Yes
No (Circle One)
Auditor:
Date:
Physician:
Specialty:
Pt. Name:
MR#:
Billed DOS:
Documented DOS:
Billed Dx Codes:
Dx 1:
Dx 2:
Dx 3:
Dx 4:
Rec Dx Codes:
Dx 1:
Dx 2:
Dx 3:
Dx 4:
E/M Service:
Billed ___________ - ______(modifier)
Recommended: ______________ - ________(modifier)
History
Physical Examination
Medical Decision Making
Constitutional:
*
HPI:
ROS:
PFSH:
GI:
Abdominal
Dx/Mgt:
*3 of :sit/stand BP, sup BP,
Location
Const.
Past Hx:
*Liver/spleen
*Hernia
Self Lim/Minor
___x1=____(Max 2)
temp, pulse rate, resp, ht, wt
*Stool Sample taken
Duration
Eyes
Meds/Allerg
Est Prob Stable
___x1=____
*general appearance
*Anus/Perineum/Rectum
Timing
ENMT
Surg/Hospital
Est Prob Worsening
___x2=____
Eyes:
GU:
Severity
Cardio
Diet
New Prob No W/U
___x3=____(Max 1)
*conjunctivae/lids
Male
Female
Quality
Resp.
Illness/Injury
New Prob Add W/U
___x4=____
*pupils/lens
*optic discs
*scrotom
*ext genitalia
Mod Factors
GI
Immun
TOTAL:
____
ENMT:
*penis
*urethra
Signs/Sympt.
GU
*ext exam ears/nose
*DRE/
*bladder
Context
Musc.
Past Social:
Data:
*ext aud canal/tymp membrane
prostate
*cervix
*hearing assessment
Integ
Marital
Lab Tests
*uterus
1
*nasal mucosa/septum/
Neuro.
Employment
*adnexa/
X-ray
1
turbinates
parametria
Psych
Occup
Med
1
*lips/teeth/gums *oropharynx
Lymphatic:
Endo
Living
Discuss test results
1
Neck:
*2 of neck,axilla,groin,other
Hem/Lym
Alcohol use
Obtain old MR
1
*neck (masses, symmetry, etc.)
Musculoskeletal:
All/Imm
Tobacco use
Case Hx-other source
2
*thyroid
*gait/station *digits/nails
All “Neg”
Education
Drs. Visual test/study
2__
Respiratory:
*exam of jt, bone,musc (1+)
Sex Hx
TOTAL:
_____
*resp effort *chest percussion
1)head/neck
*chest palpation
2)spine/rib/pelvis 3-4)rt/lt
*auscultation lungs
Physical Presence:
Family
upper ext 5-6)rt/lt low ext
Documented by:
Cardiovascular:
Skin:
Clearly Documented
Attending Only
*palpation heart
*inspect skin/subc tissue
Not Documented
Attending with
*auscultation
*palpation skin/subc tissue
Resident
Co-signature
exam of * carotid arteries
Neurologic:
Medical Student
Electronic Signature
* femoral arteries
*cranial nerves *sensation
Other: __________
Unclear
* abdominal aorta
*deep tendon reflexes
Consults:
Documented - not
* pedal pulses
Other:
Psychiatric:
signed by Attending
* extremities
*judgment/insight
Request in
E/M Criteria:
Chest: *inspection breast
Render Opinion?
Yes
MSE: *orientation
record?
Time as E/M factor:
* palpation breast/axillae
*remote &recent memory
General Multi-specialty
No
If Yes, explain:
*mood & affect
Yes
Specialty exam: (see
____________________
Report
attached) ___________
Yes
No
Provided?
No
FOC
EXP
DET
COMP
HX:
Foc
Exp
Detail
Comp
MDM
Sfwd
Low
Mod
High
1-5
At least
12 elements
18 or all
HPI
1-3
1-3
>3
>3
Dx/Mgt
0-1
2
3
>3
elements
6 elements
shaded
ROS
0
1
2-9
10+
Data:
0-1
2
3
>3
1 body/organ
2-7 body/org
2-7 body/org
8+ org system
PFSH
0
0
1
2 or 3
Risk:
Min
Low
Mod
High
1
ADVERTISEMENT
0 votes
Related Articles
Related forms










Related Categories
Parent category: Medical