Elfin Form 02 - Infant Daily Dosing Log (34 Postmenstrual Weeks Of Age) Page 2
ADVERTISEMENT
 Printable pdf") 1
1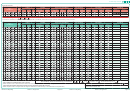 2
2ELFIN study number:
Example section:
Feeds
Form 3/4
Dose to be administered
Accountability
Preparation
Signatures
Not
Date
*Antibiotics/
Feeds
Working weight
Dose
Dose
Pots
Pots
Add 4 mL
Add 1 mL
Stand for 30
Given in
given
r
(DD/MM/YY)
Breast
Formula
PN
Nurse 1
Nurse 2
Antifungals
(Kg)
In mg
In mL
used
wasted
water
milk
min
next 30 min
stopped
.
.
/
/
0 7
0 2
1 4
0
9 8
1 4 7
1
9
1
D
D
M
M
Y Y
.
.
/
/
0 8
0 2
1 4
D
D
M
M
Y Y
/
/
Last dose to be given on:
.
D
D
M
M
Y Y
This date is calculated at randomisation and corresponds to 34 weeks’ postmenstrual age. Refer to randomisation print out for date.
Feeds
Form 3/4
Dose to be administered
Accountability
Preparation
Signatures
Not
Date
*Antibiotics/
Feeds
Working weight
Dose
Dose
Pots
Pots
Add 4 mL
Add 1 mL
Stand for
Given in
given
r
(DD/MM/YY)
Breast
Formula
PN
Nurse 1
Nurse 2
Antifungals
stopped
(Kg)
In mg
In mL
used
wasted
water
milk
30 min
next 30 min
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
.
.
/
/
D
D
M
M
Y Y
Accountability check at end of dosing, or at transfer:
+
+
unused = 24:
or indicate discrepancy:
*
Tick if antibiotics or antifungals were given on this day
Number of pots from this pack transferred to continuing care
(Please complete a Form 3: Late-Onset Invasive Infection if 5 consecutive days of antibiotics or antifungals are given, or if this infant died from suspected infection)
r
Tick if feeds were stopped or withheld for more than 4 hours for suspected or proven NEC on this day
Infant transferred to site:
(Please complete a Form 4: Gut Signs if feeds are stopped or withheld for 5 consecutive days, or if this infant died from suspected NEC)
ELFIN Form 2: Daily Dosing
Version 2.0, 18 August 2015
Page 2 of 4
ELFIN Form 2: Daily Dosing
Version 2.0, 18 August 2015
Page 3 of 4
ADVERTISEMENT
0 votes
Related Articles
Related forms





 Form - Michigan")




Related Categories
Parent category: Medical