Tb Contact Investigation Form
ADVERTISEMENT
 1
1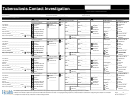 2
2Report and Date
____/____/____
Initial
Tuberculosis Contact Investigation
____/____/____
Update
LOC L HEAL
A
TH DEPARTMENT
____/____/____
Final
Case Manager_________________________________________
State Case#_________________________________
Local Case#________________________________
CASE INFORMATION
Disease Site
Need for Contact Investigation (case characteristics)
Sputum Smear Positive Cases
High
Name (last, first, MI)____________________________________
Pulmonary, Pleural,
(sputum-smear pos and/or cavitary or laryngeal TB)
Contacts offered RIF
Med
Laryngeal
(sputum-smear neg, culture positive pulmonary or pleural TB)
for pilot project?
Low
Date of Birth ____/____/______
Other
(sputum-smear neg, culture negative pulmonary or pleural TB)
None
(all others, no pulmonary TB, contact investigation not needed)
Infectious Period
Start Date____/____/____
End Date____/____/____
Pending
CONTACT* INFORMATION
≥ 8 week TST/QFT
Contact Risks
Symptoms <8 week TST/QFT
CXR
LTBI Treatment
Final Status***
High Risk of Infection
Low Risk of Infection
Yes
TST:
TST:
Date Started
Finished LTBI Tx
____/____/____ ____/____/____ ____/____/____ ____/____/____
First Name _______________________________
Household
No risk
No
TB Disease
Last Name _______________________________
Age<5
Other low risk
TST mm________
TST mm________
Negative
Died
Address _________________________________
HIV/AIDS
___________
QFT:
QFT:
Abnormal
Date Stopped
Refused
____/____/____ ____/____/____
____/____/____
Phone___________________________________
CXR c/w Inactive TB
TB disease
Lost
Date of Birth ____/____/______
Congregate Setting
Result:____________
Result:____________
Abnormal
Regimen:
Moved_________
Country of Birth______________ DOE ____/____
Country of
Birth
______________ DOE ____ _
/
___
Exceeds
Exceeds Exposure
Exposure
inactive
inactive TB
TB
INH
INH
Adverse Tx Rxn
Adverse Tx
Rxn
Date Last Exposed ____/____/____ or
ongoing
Other Medical Risk
Prior TST/QFT+__________
_________________
Rif
Other Provider
Other_______________
Prior TX_________________
_________________
Other_________
Decision ______
High Risk of Infection
Low Risk of Infection
Yes
TST:
TST:
Date Started
Finished LTBI Tx
____/____/____ ____/____/____ ____/____/____ ____/____/____
First Name _______________________________
Household
No risk
No
TB Disease
Last Name _______________________________
Age<5
Other low risk
TST mm________
TST mm________
Negative
Died
Address _________________________________
HIV/AIDS
___________
QFT:
QFT:
Abnormal
Date Stopped
Refused
____/____/____ ____/____/____
____/____/____
Phone___________________________________
CXR c/w Inactive TB
TB disease
Lost
Date of Birth ____/____/______
Congregate Setting
Result:____________
Result:____________
Abnormal
Regimen:
Moved_________
Country of Birth______________ DOE ____/____
Exceeds Exposure
inactive TB
INH
Adverse Tx Rxn
Date Last Exposed ____/____/____ or
ongoing
Other Medical Risk
Prior TST/QFT+__________
_________________
Rif
Other Provider
Other_______________
Prior TX_________________
_________________
Other_________
Decision ______
High Risk of Infection
Low Risk of Infection
Yes
TST:
TST:
Date Started
Finished LTBI Tx
____/____/____ ____/____/____ ____/____/____ ____/____/____
First Name _______________________________
Household
No risk
No
TB Disease
Last Name _______________________________
Age<5
Other low risk
TST mm________
TST mm________
Negative
Died
Address _________________________________
HIV/AIDS
___________
QFT:
QFT:
Abnormal
Date Stopped
Refused
____/____/____ ____/____/____
____/____/____
Phone___________________________________
CXR c/w Inactive TB
TB disease
Lost
Date of Birth ____/____/______
Congregate Setting
Result:____________
Result:____________
Abnormal
Regimen:
Moved_________
Country of Birth______________ DOE ____/____
Exceeds Exposure
inactive TB
INH
Adverse Tx Rxn
Date Last Exposed ____/____/____ or
ongoing
Other Medical Risk
Prior TST/QFT+__________
_________________
Rif
Other Provider
Other_______________
Prior TX_________________
_________________
Other_________
Decision ______
* A contact is a person whom the health department believes had significant exposure,and for whom enough identifying/contacting information is available.
Page 1 of _____
** Relative risk of infection depends on exposure and medical risk factors of the contact. For congregate setting exposures, contact the State for assistance in categorizing the contact's risk of infection.
Revised 8/4/2011
*** Complete for contacts not fully evaluated or contacts starting treatment
ADVERTISEMENT
0 votes
Related Articles
Related forms










Related Categories
Parent category: Medical