National Sleep Foundation Sleep Diary Template Page 2
ADVERTISEMENT
 1
1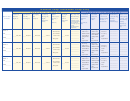 2
2National Sleep Foundation Sleep Diary
C O M P L E T E A T E N D O F D A Y
C O M P L E T E I N M O R N I N G
I went to
I got out of
Last night,
I woke up
When I
Last night
My sleep was
I consumed
I exercised
Approximatel
Medication(s)
About 1 hour
bed last
bed this
I fell
during the
woke up for
I slept a
caffeinated
at least 20
y 2-3 hours
I took during
before going
disturbed by:
Fill out days
night at:
morning at:
asleep in:
night:
the day, I
total of:
drinks in
minutes
before going
the day:
to sleep, I did
5-7 below
(List any mental,
felt:
the:
in the:
to bed, I
the following
emotional, physical
(Record number
(Record number
[List name of
consumed:
activity:
or environmental fac-
of times)
of hours)
medication/drug(s)]
(e.g. coffee, tea,
(Check one)
tors that affected
cola)
(List activity; e.g.
your sleep; e.g. stress,
snoring,
watch TV, work,
physical discomfort,
read)
temperature)
Morning
Morning
____________
____________
____________
DAY 5
Refreshed
Afternoon
Afternoon
Alcohol
____________
____________
____________
Within several
A heavy
Within several
DAY________
Somewhat
hours before
____PM/AM
____PM/AM
___Minutes
____Times
____Hours
hours before
meal
____________
____________
____________
refreshed
going to bed
going to bed
Not
DATE_______
____________
____________
____________
Fatigued
Not
applicable
Not
____________
____________
____________
applicable
applicable
Morning
Morning
____________
____________
____________
DAY 6
Refreshed
Afternoon
Afternoon
Alcohol
____________
____________
____________
Within several
A heavy
Within several
DAY________
Somewhat
hours before
meal
____PM/AM
____PM/AM
___Minutes
____Times
____Hours
hours before
____________
____________
____________
refreshed
going to bed
Not
going to bed
DATE_______
____________
____________
____________
Fatigued
Not
applicable
Not
____________
____________
____________
applicable
applicable
Morning
Morning
____________
____________
____________
DAY 7
Refreshed
Afternoon
Afternoon
Alcohol
____________
____________
____________
Within several
A heavy
Within several
DAY________
Somewhat
hours before
meal
____PM/AM
____PM/AM
___Minutes
____Times
____Hours
hours before
____________
____________
____________
refreshed
going to bed
Not
going to bed
DATE_______
____________
____________
____________
Fatigued
Not
applicable
Not
____________
____________
____________
applicable
applicable
ADVERTISEMENT
0 votes
Related Articles
Related forms










Related Categories
Parent category: Life