Girl Scouts Of Northern California Camper Health Record And Emergency Information Form Page 2
ADVERTISEMENT
 1
1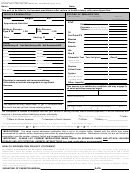 2
2Girl Scouts of Northern California
CAMPER HEALTH RECORD AND EMERGENCY INFORMATION (page 2 of 2)
Name:
Date:
This part to be filled in by licensed practitioner after review of health history with parent/guardian
HEALTH EXAMINATION
RECORD OF IMMUNIZATION
Immunization
Year Primary
Year of
Height
Weight
B.P.
Series Completed
Last Booster
DTaP
Appearance-Nutrition
Diphtheria
Pertussis
(Whooping Cough)
Without Glasses:
With Glasses:
Tetanus
(within last 10 years)
Eyes R 20/
L 20/
R 20/
L 20/
Td
Oral Polio/IPV
Ears
Hearing R
L
Measles
Mumps
CODE:
Satisfactory=S
Not Satisfactory=NS Not Examined=NE
Rubella
Hib
Nose
Throat
Hep B
Teeth
Heart
Lungs
Abdomen
Tuberculin Test Year last given
Result
Genitalia
Hernia
Typhoid and
Paratyphoid
Skin
Musculoskeletal
Cholera
General physical and emotional status
Yellow Fever
Urinalysis*
HGB*
Other notes
Typhus
Rocky Mountain
Spotted Fever
Physician’s comments and recommendations.
Other: (specify)
Give details or indicate management or significant
illnesses.
This person is in satisfactory condition and may engage in
all usual activities except as noted.
Licensed Practioner's Signature
(Print) Licensed Practioner's Name
Address/City/State/Zip
E-Mail
*Not required for every health exam. A girl 11-18 should have
Area Code + Phone
FAX: Area Code + Phone
Date
this test if she has not had it since entering puberty.
(
)
(
)
This information is needed to measure how well your council is serving the Bay Area’s diverse population, it will be combined with
everyone in the troop without identifying anyone individually.
Asian
The girl’s racial background is:
American Indian or Alaskan Native
(please check as many as apply)
Black or African American
Hawaiian or Pacific Islander
White
Other(
_________________
specify)
The girl’s ethnic background is:
Hispanic or Latino
Not Hispanic or Latino
(please check one)
Is your girl/ward disabled?
NO
YES If YES, does she need accommodation?
NO
YES If YES, attach a separate paper to explain.
MEDICATIONS: The camp cannot administer medication that is not in its original bottle, labeled with the child’s own name,
accompanied by specific written dispensing instructions by parent/guardian or physician. Medications include, but are not limited to:
prescription, over the counter, vitamins, herbal and homeopathic remedies.
IMPORTANT: PLEASE LIST CURRENT MEDICATIONS BEING TAKEN ON SEPARATE PAPER AND ATTACH—INCLUDE
DOSAGE AND ANY POTENTIAL HARMFUL INTERACTIONS (e.g. food, medications, environmental)
HEALTH INFORMATION PRIVACY STATEMENT
The Camper Health Record and Emergency Information is for health care concerns at the specified event only. All records will be handled by
staff/volunteers whose job includes processing or using this information for the benefit of the participant. All medical records will be held in limited
access by the health care supervisor of the specific event. Minimal necessary information may be shared with event staff/volunteers in order to provide
adequate participant safety and health care. The Camper Health Record and Emergency Information will be retained by the sponsoring council or
GSUSA until it is destroyed. All forms/records with noted treatment will be retained for seven years past the age of maturity of the participant. Access
to the information will be limited, but copies may be requested from the event sponsor, by the participant or their legal representative.
I have read the above procedures for handling the health form information and I agree to the release of any records necessary for treatment, referral,
billing or insurance purposes.
SIGNATURE OF PARENT/GUARDIAN:
DATE:
ADVERTISEMENT
0 votes
Related Articles
Related forms










Related Categories
Parent category: Business