Immunization Schedule For Children And Adolescents Aged 18 Years Or Younger Page 7
ADVERTISEMENT
 1
1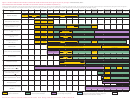 2
2 3
3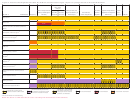 4
4 5
5 6
6 7
7 8
8For further guidance on the use of the vaccines mentioned below, see:
• For other catch-up guidance, see Figure 2.
Catch-up vaccination
vaccination of persons with high-risk conditions and
:
7.
Influenza vaccines. (Minimum age: 6 months for inacti-
• Ensure that all persons aged 7 through 18 years without
other persons at increased risk” and “Meningococcal B
vated influenza vaccine [IIV], 18 years for recombinant
evidence of immunity (see MMWR 2007;56[No. RR-4],
vaccination of persons with high-risk conditions and other
influenza vaccine [RIV])
available at
persons at increased risk of disease” below.
Routine vaccination:
) have 2 doses of
Catch-up vaccination:
• Administer influenza vaccine annually to all children
varicella vaccine. For children aged 7 through 12 years,
• Administer Menactra or Menveo vaccine at age 13 through
beginning at age 6 months. For the 2016–17 season,
the recommended minimum interval between doses is
18 years if not previously vaccinated.
use of live attenuated influenza vaccine (LAIV) is not
3 months (if the second dose was administered at least 4
• If the first dose is administered at age 13 through 15 years,
recommended.
weeks after the first dose, it can be accepted as valid); for
a booster dose should be administered at age 16 through
For children aged 6 months through 8 years
persons aged 13 years and older, the minimum interval
18 years, with a minimum interval of at least 8 weeks
:
• For the 2016–17 season, administer 2 doses (separated by
between doses is 4 weeks.
between doses.
at least 4 weeks) to children who are receiving influenza
10. Hepatitis A (HepA) vaccine. (Minimum age: 12 months)
• If the first dose is administered at age 16 years or older, a
vaccine for the first time or who have not previously
Routine vaccination
booster dose is not needed.
:
received ≥2 doses of trivalent or quadrivalent influenza
• Initiate the 2-dose HepA vaccine series at ages 12 through
• For other catch-up guidance, see Figure 2.
vaccine before July 1, 2016. For additional guidance,
23 months; separate the 2 doses by 6 to 18 months.
Clinical discretion:
follow dosing guidelines in the 2016–17 ACIP influenza
• Children who have received 1 dose of HepA vaccine
• Young adults aged 16 through 23 years (preferred age
vaccine recommendations (see MMWR August 26,
before age 24 months should receive a second dose 6 to
range is 16 through 18 years) who are not at increased
2016;65(5):1-54, available at
18 months after the first dose.
risk for meningococcal disease may be vaccinated with a
).
• For any person aged 2 years and older who has not
2-dose series of either Bexsero (0, ≥1 month) or Trumenba
• For the 2017–18 season, follow dosing guidelines in the
already received the HepA vaccine series, 2 doses of
(0, 6 months) vaccine to provide short-term protection
2017–18 ACIP influenza vaccine recommendations.
HepA vaccine separated by 6 to 18 months may be
against most strains of serogroup B meningococcal
For persons aged 9 years and older:
administered if immunity against hepatitis A virus
disease. The two MenB vaccines are not interchangeable;
• Administer 1 dose.
infection is desired.
the same vaccine product must be used for all doses.
8.
Measles, mumps, and rubella (MMR) vaccine. (Minimum
Catch-up vaccination
• If the second dose of Trumenba is given at an interval of
:
age: 12 months for routine vaccination)
• The minimum interval between the 2 doses is 6 months.
<6 months, a third dose should be given at least 6 months
Routine vaccination
Special populations
after the first dose; the minimum interval between the
:
:
• Administer a 2-dose series of MMR vaccine at ages 12
• Administer 2 doses of HepA vaccine at least 6 months apart
second and third doses is 4 weeks.
through 15 months and 4 through 6 years. The second
to previously unvaccinated persons who live in areas where
Meningococcal conjugate ACWY vaccination of persons
with high-risk conditions and other persons at increased
dose may be administered before age 4 years, provided at
vaccination programs target older children, or who are at
least 4 weeks have elapsed since the first dose.
increased risk for infection. This includes persons traveling
risk:
• Administer 1 dose of MMR vaccine to infants aged 6
to or working in countries that have high or intermediate
Children with anatomic or functional asplenia (including
through 11 months before departure from the United
endemicity of infection; men having sex with men; users
sickle cell disease), children with HIV infection, or children
States for international travel. These children should be
of injection and non-injection illicit drugs; persons who
with persistent complement component deficiency
revaccinated with 2 doses of MMR vaccine, the first at age
work with HAV-infected primates or with HAV in a research
(includes persons with inherited or chronic deficiencies
12 through 15 months (12 months if the child remains in
laboratory; persons with clotting-factor disorders; persons
in C3, C5-9, properdin, factor D, factor H, or taking
an area where disease risk is high), and the second dose at
with chronic liver disease; and persons who anticipate
eculizumab [Soliris]):
least 4 weeks later.
close, personal contact (e.g., household or regular
▪ Menveo
• Administer 2 doses of MMR vaccine to children aged
babysitting) with an international adoptee during the first
ɱ Children who initiate vaccination at 8 weeks. Administer
12 months and older before departure from the United
60 days after arrival in the United States from a country
doses at ages 2, 4, 6, and 12 months.
States for international travel. The first dose should be
with high or intermediate endemicity. The first dose should
ɱ Unvaccinated children who initiate vaccination at 7
administered on or after age 12 months and the second
be administered as soon as the adoption is planned, ideally,
through 23 months. Administer 2 primary doses, with
dose at least 4 weeks later.
2 or more weeks before the arrival of the adoptee.
the second dose at least 12 weeks after the first dose
Catch-up vaccination
11. Meningococcal vaccines. (Minimum age: 6 weeks for
:
AND after the first birthday.
• Ensure that all school-aged children and adolescents
Hib-MenCY [MenHibrix], 2 months for MenACWY-CRM
ɱ Children 24 months and older who have not received a
have had 2 doses of MMR vaccine; the minimum interval
[Menveo], 9 months for MenACWY-D [Menactra], 10 years
complete series. Administer 2 primary doses at least 8
between the 2 doses is 4 weeks.
for serogroup B meningococcal [MenB] vaccines: MenB-
weeks apart.
9.
Varicella (VAR) vaccine. (Minimum age: 12 months)
4C [Bexsero] and MenB-FHbp [Trumenba])
▪ MenHibrix
Routine vaccination
Routine vaccination:
:
ɱ Children who initiate vaccination at 6 weeks. Administer
• Administer a 2-dose series of VAR vaccine at ages 12
• Administer a single dose of Menactra or Menveo vaccine
doses at ages 2, 4, 6, and 12 through 15 months.
through 15 months and 4 through 6 years. The second
at age 11 through 12 years, with a booster dose at age 16
ɱ If the first dose of MenHibrix is given at or after age 12
dose may be administered before age 4 years, provided
years.
months, a total of 2 doses should be given at least 8
at least 3 months have elapsed since the first dose. If the
• For children aged 2 months through 18 years with high-
weeks apart to ensure protection against serogroups
second dose was administered at least 4 weeks after the
risk conditions, see “Meningococcal conjugate ACWY
C and Y meningococcal disease.
first dose, it can be accepted as valid.
ADVERTISEMENT
0 votes
Related Articles
Related forms



 - Schedule For Calculating The Nonresident Credit Part-year Residents, Nonresidents And") Schedule Nr (form 1040me) - Schedule For Calculating The Nonresident Credit Part-year Residents, Nonresidents And "safe Harbor" Residents Only - 2015
Financial
Schedule Nr (form 1040me) - Schedule For Calculating The Nonresident Credit Part-year Residents, Nonresidents And "safe Harbor" Residents Only - 2015
Financial
 - Schedule For Calculating The Nonresident Credit Part-year Residents, Nonresidents And") Schedule Nr (form 1040me) - Schedule For Calculating The Nonresident Credit Part-year Residents, Nonresidents And "safe Harbor" Residents Only - 2012
Financial
Schedule Nr (form 1040me) - Schedule For Calculating The Nonresident Credit Part-year Residents, Nonresidents And "safe Harbor" Residents Only - 2012
Financial
 - Schedule For Calculating The Nonresident Credit Part-year Residents, Nonresidents And") Schedule Nr (form 1040me) - Schedule For Calculating The Nonresident Credit Part-year Residents, Nonresidents And "safe Harbor" Residents Only - 2012
Financial
Schedule Nr (form 1040me) - Schedule For Calculating The Nonresident Credit Part-year Residents, Nonresidents And "safe Harbor" Residents Only - 2012
Financial
 - Schedule For Calculating The Nonresident Credit Part-year Residents, Nonresidents And")



Related Categories
Parent category: Medical