Form Cms-416 - Annual Early Ad Periodic Screening Diagnostic And Treatment Participation Report
ADVERTISEMENT
 1
1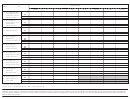 2
2DEPARTMENT OF HEALTH AND HUMAN SERVICES
Form Approved
CENTERS FOR MEDICARE & MEDICAID SERVICES
OMB No. 0938-0354
FORM CMS-416: ANNUAL EPSDT PARTICIPATION REPORT
Age Groups
State ___________FY _______
Total
<1
1–2*
3–5
6–9
10–14
15–18
19–20
1. Total Individuals
CN
Eligible for EPSDT
MN
TOTAL
2a. State Periodicity
Schedule
2b. Number of Years
in Age Group
1
2
3
4
5
4
2
2c. Annualized State
Periodicity Schedule
3a. Total Months
CN
of Eligibility
MN
TOTAL
3b. Average Period
CN
of Eligibility
MN
TOTAL
4. Expected Number of
CN
Screenings per
MN
Eligible
TOTAL
5. Expected Number
CN
of Screenings
MN
TOTAL
6. Total Screens
CN
Received
MN
TOTAL
CN
7. Screening Ratio
MN
TOTAL
* Includes 12–month visit
Note: “CN” - Categorically Needy, “MN” = Medically Needy
Form CMS-416 (06/99)
ADVERTISEMENT
0 votes
Related Articles
Related forms
 - West Virginia Department Of Health And Human Resources Early And Periodic Screening, Diagnosis, And Treatment (epsdt)") 18 Month Form (healthcheck Program Preventive Health Screen) - West Virginia Department Of Health And Human Resources Early And Periodic Screening, Diagnosis, And Treatment (epsdt)
Life
18 Month Form (healthcheck Program Preventive Health Screen) - West Virginia Department Of Health And Human Resources Early And Periodic Screening, Diagnosis, And Treatment (epsdt)
Life
 Form Cms-3070g - Intermediate Care Facilities For Individuals With Intellectual Disabilities Survey Report
Medical
Form Cms-3070g - Intermediate Care Facilities For Individuals With Intellectual Disabilities Survey Report
Medical


 Form Dfc-f5-dwc-25 - Florida Workers' Compensation Uniform Medical Treatment/ Status Reporting Form
Legal
Form Dfc-f5-dwc-25 - Florida Workers' Compensation Uniform Medical Treatment/ Status Reporting Form
Legal
 Form Rpd-41359 - Annual Withholding Of Net Income From A Fiduciary Detail Report - New Mexico Taxation And Revenue Department - 2014
Financial
Form Rpd-41359 - Annual Withholding Of Net Income From A Fiduciary Detail Report - New Mexico Taxation And Revenue Department - 2014
Financial
 Form Cms-1856 - Request For Certification In The Medicare And/or Medicaid Program To Provide Outpatient Physical Therapy And/or Speech Pathology Services
Medical
Form Cms-1856 - Request For Certification In The Medicare And/or Medicaid Program To Provide Outpatient Physical Therapy And/or Speech Pathology Services
Medical



Related Categories
Parent category: Medical