Form 13441-A - Health Coverage Tax Credit (Hctc) Monthly Registration And Update Page 3
Download a blank fillable Form 13441-A - Health Coverage Tax Credit (Hctc) Monthly Registration And Update in PDF format just by clicking the "DOWNLOAD PDF" button.
Open the file in any PDF-viewing software. Adobe Reader or any alternative for Windows or MacOS are required to access and complete fillable content.
Complete Form 13441-A - Health Coverage Tax Credit (Hctc) Monthly Registration And Update with your personal data - all interactive fields are highlighted in places where you should type, access drop-down lists or select multiple-choice options.
Some fillable PDF-files have the option of saving the completed form that contains your own data for later use or sending it out straight away.
ADVERTISEMENT
 Monthly Registration And Update Printable pdf") 1
1 2
2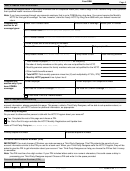 3
3 4
4Your SSN
Page 3
Part 4: Health Plan Information
Fill out the information below. If your family members are on a separate health plan, make a copy of Part 4 before filling it out to provide
their qualified health insurance information.
Note: If you have coverage through your spouse’s employer that is not a COBRA plan, stop here. You cannot receive the Monthly
HCTC for this type of coverage. You can, however, claim the Yearly HCTC by filing Form 8885 with your federal income tax
return.
Health Plan Provider name
Effective date of coverage
Health plan ID number
Complete this
section for all
coverage types:
HCTC vendor name
(name of company to be payed on your behalf)
HCTC vendor number
(contact your Health Plan Provider or Third Party Administrator)
Provide at least one of the following ID Numbers.
Member ID
Group ID
Policy or plan ID
Policy holder’s name
Policy holder’s SSN
Total monthly premium
(First, Middle Initial, Last, Suffix)
1. Total number of people
on this policy
(you and any family members)
2. Number of family members on this policy who are not qualified for the HCTC
3. Monthly premium amount for family members who are not qualified for the HCTC
4. Other health benefits amount
5. Total HCTC Total monthly premium minus line (3) and multiplied by 27.5% (.275)
6. Monthly HCTC payment Line 4 plus Line 5
Former employer
Former employer’s HR telephone number
Complete this
section only if you
have COBRA
Start Date for COBRA Coverage
End Date for COBRA Coverage
coverage:
(mm/dd/yyyy)
(mm/dd/yyyy)
Check here if this is a Lifetime Benefit.
Part 5: Account Accessibility
If you would like to allow someone else – for example, your spouse, family member, or other trusted advisor – to have access to your
account information, please complete this page. This person, called a Third-Party-Designee, will be able to ask questions about, or
make changes to, your HCTC account or personal information, as appropriate.
Third-Party-Designee
Do you want to allow another person to talk with the HCTC Program about your account?
Yes. Complete the rest of this page and choose a PIN.
No. Go to Part 6 to sign and date the HCTC Monthly Registration and Update form.
Name of Third-Party-Designee
(First, Middle Initial, Last, Suffix)
Primary telephone number
Alternate telephone number
Personal Identification Number (PIN)
IMPORTANT! You must choose a PIN when you make someone a Third-Party-Designee. This PIN protects the security of your
account information similar to the PIN you use for a bank card. When your Third-Party-Designee calls the HCTC Program, they will be
asked to give the PIN to get information about your account. Your Third-Party-Designee can help you choose the PIN so that it is easy
to remember.
Note: The PIN must be a five-digit number. If your PIN includes letters and/or non-numeric characters, this could cause a delay in
processing your Third-Party-Designee request. Choose a PIN and write it in the space provided.
Personal Identification Number (PIN)
13441-A
Catalog Number 57559E
Form
(Rev. 5-2017)
ADVERTISEMENT
0 votes
Related Articles
Related forms
 Monthly Registration And Update")
 Reimbursement Request Form")
 Advance Payments - 2018")
 Advance Payments - 2017")
 Advance Payments - 2013")
 Advance Payments - 2013")
 Advance Payments - 2012")
 Advance Payments - 2016")
 Reimbursement Request Form")
 Blank Payment Coupon")
Related Categories
Parent category: Financial