Minnesota Life Group Life Insurance Evidence Of Insurability Form Page 2
Download a blank fillable Minnesota Life Group Life Insurance Evidence Of Insurability Form in PDF format just by clicking the "DOWNLOAD PDF" button.
Open the file in any PDF-viewing software. Adobe Reader or any alternative for Windows or MacOS are required to access and complete fillable content.
Complete Minnesota Life Group Life Insurance Evidence Of Insurability Form with your personal data - all interactive fields are highlighted in places where you should type, access drop-down lists or select multiple-choice options.
Some fillable PDF-files have the option of saving the completed form that contains your own data for later use or sending it out straight away.
ADVERTISEMENT
 1
1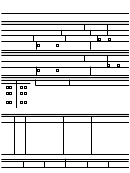 2
2 3
3abcd
Group Life Insurance Evidence of Insurability
A
A
A
Minnesota Life Insurance Company - A Securian Company
400 Robert Street North
B1-3102
St. Paul, Minnesota 55101-2098
Fax 651-665-7092
EMPLOYER NAME: State of New Mexico
POLICY NUMBER: 34426
EMPLOYEE INFORMATION
(always complete for coverage that requires evidence of insurability)
First name
Middle initial
Last name
Evening phone number
Daytime phone number
Street address
City
State
Zip code
Date of birth
Employee ID
Date of employment
Gender
Male
Female
Total amount of Additional Employee
What is the reason for your coverage election or increase? Email address
Life insurance requested
Newly Eligible
Family Status Change
Date of the event:
SPOUSE/DOMESTIC PARTNER INFORMATION
(only complete if coverage requires evidence of insurability)
First name
Middle initial
Last name
Daytime phone number
Evening phone number
Gender
Date of birth
Female
Male
Email address
Total amount of Spouse/Domestic
What is the reason for your coverage election or increase?
Partner Life insurance requested
Newly Eligible
Family Status Change
$
Date of the event:
HEALTH QUESTIONS
(always complete for coverage that requires evidence of insurability)
Employee
Spouse/domestic partner
Employee
Spouse/DP
Occupation
Height
Weight
Height
Weight
Yes No
Yes No
1. During the past three years, have you for any reason consulted a physician(s) or
other health care provider(s) or been hospitalized?
2. Have you ever had, or been treated for, any of the following: heart, lung, kidney, liver,
nervous system, or mental disorder; high blood pressure; stroke; diabetes; cancer or
tumor; drug or alcohol abuse including addiction?
3. Have you ever been diagnosed as having Acquired Immune Deficiency Syndrome
(AIDS), or any disorder of your immune system; or had any test showing evidence of
antibodies to the AIDS virus (a positive HIV test)?
If you answer "Yes" to any question, please provide additional information below or on a separate sheet of paper.
ADDITIONAL HEALTH INFORMATION
(provide details for every "Yes" answer to the health questions)
REASON FOR
NAME AND ADDRESS OF DOCTOR,
NAME
DATE
DIAGNOSIS AND TREATMENT
CONSULTATION
CLINIC, HOSPITAL
FOR OFFICE USE ONLY:
Additional Employee Life
Spouse/Domestic Partner Life
Current in force
Current in force
U/W applied for
Total elected
U/W applied for
Total elected
$
$
$
$
$
$
BBBBBB
BBBBBB
PLEASE READ & SIGN NEXT PAGE & SEND ALL PAGES TO MINNESOTA LIFE
12-31468.30
EdF83454 Rev 7-2015
ADVERTISEMENT
0 votes
Related Articles
Related forms










Related Categories
Parent category: Legal