Newborn Orders - Saskatoon Health Region
ADVERTISEMENT
 1
1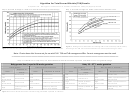 2
2 3
3PATIENT IDENTIFICATION
RUH
SCH
SPH
OTHER:
ACTION
Newborn Admission Order Set for Maternal and Newborn Care Unit
Admit to:
Diagnosis:
Weight: _____kg
Prevention of Ophthalmia Neonatorum
erythromycin ophthalmic ointment (5 mg/g) to each eye X 1 dose (give in Labour & Birth unit)
Prevention of Hemorrhagic Disease of the Newborn
vitamin K 1 mg IM X 1 dose (give in Labour & Birth unit)
Prevention of Maternal to Newborn Transmission of Hepatitis B
If positive or unknown maternal Hepatitis B surface antigen (HBsAg), administer Hepatitis B
vaccine 0.5 mL IM within 12 hours of birth per protocol (either Recombivax HB 5 micrograms/0.5
mL OR Engerix-B 10 micrograms/0.5 mL)
If positive maternal HBsAg administer Hepatitis B Immune Globulin (HBIg) 0.5 mL IM as soon as
possible after birth
Jaundice and Newborn Metabolic Screening
Abbreviations: Total Serum Bilirubin (TSB), Transcutaneous Bilirubin (TcB), Direct Antiglobulin Test (DAT)
6/7
MRP to specify: Gestational Age:
35 – 37
weeks
greater than / equal to 38 weeks
MRP to specify: Risk Factors:
No
Yes (e.g. isoimmune hemolytic disease, G6PD, asphyxia,
respiratory distress, significant lethargy, temperature instability, sepsis, acidosis)
Follow Maternal Newborn Unit Policy: Newborn Transcutaneous Bilirubin Screening #406-1
If Newborn jaundiced prior to 24 hours of age, obtain TSB and DAT; notify MRP
Obtain DAT when indicated below if DAT unknown
TcB Screening: Do TcB prior to Metabolic Screen, once daily and within 4 hours of discharge.
See gestation-specific TcB nomogram (Figure 4). Do TSB and DAT if indicated and notify MRP.
If phototherapy recommended based on TSB and DAT, gestational age and known risk
factors (Figure 1 on reverse); notify MRP and initiate phototherapy
If TSB does not indicate phototherapy, repeat TcB in 24 hours
If TSB not indicated, use TcB Nomogram (Figure 4) to determine discharge follow-up advised
TSB Screening: If TcB will delay care or unavailable, obtain TSB with Newborn Screen
If phototherapy recommended based on TSB, gestational age and known risk factors (Figure
1 on reverse); notify MRP, initiate phototherapy and obtain DAT with next blood work
If TSB does not indicate phototherapy, use TSB zone graph to determine need for further
testing and discharge follow-up advised (Figure 2 and 3 on reverse)
Note: DAT advised if Newborn jaundiced and mom blood group O, TSB in high zone, TSB in low intermediate or high
intermediate zone and infant is less than 38 weeks, if further treatment or testing advised (see Figure 1)
PRACTITIONER PRINTED NAME
PRACTITIONER SIGNATURE
DATE/TIME
Notice of confidentiality: Contains information that is time sensitive or confidential. Use, disclosure, copying or communication of the contents is prohibited. If
you have received in error, notify the SHR Pharmacy Manager, Operations (306-655-6695).
Form #100322
12/15
Category: Orders
Page 1 of 2
NEWBORN
ADVERTISEMENT
0 votes
Related Articles
Related forms


")







Related Categories
Parent category: Business