Intranasal Vaccine Consent Form - Kanawha-Charleston Health Department Page 2
ADVERTISEMENT
 1
1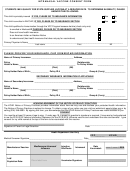 2
2INTRANASAL VACCINE CONSENT FORM
STUDENTS MAY QUALIFY FOR STATE-SUPPLIED VACCINE AT A REDUCED RATE. TO DETERMINE ELIGIBILITY, PLEASE
ANSWER THE FOLLOWING:
This child is privately insured IF YES, PLEASE GO TO INSURANCE INFORMATION
Yes
No
This child is enrolled in WVCHIP, IF YES, PLEASE GO TO INSURANCE SECTION
Yes
No
This child qualifies for Immunization through the VFC Program because he/she (check only one):
Is enrolled in Medicaid IF CHECKED, PLEASE GO TO INSURANCE SECTION
Does not have health insurance
Is an American Indian or Alaskan Native
Is underinsured (has health insurance that does not pay for vaccinations)
Primary Physician’s Name____________________________________________________________________________________
Last name
First
MI
PLEASE PROVIDE YOUR INSURANCE, CHIP OR MEDICAID INFORMATION
Name of Primary Insurance: _____________________________________ Address______________________________________
Policy
Relationship
Holder’s Name __________________________________________________ To Policy Holder
_______________________
(Last)
(First)
(MI)
Policy Holder Date of Birth:________________ Policy ID # ________________________ Group # (if any) __________________
SECONDARY INSURANCE INFORMATION IF APPLICABLE
Name of Secondary Insurance: __________________________________ Address______________________________________
Policy
Relationship
Holder’s Name __________________________________________________ To Policy Holder
_______________________
(Last)
(First)
(MI)
Policy Holder Date of Birth:________________ Policy ID # ________________________ Group # (if any) __________________
ACKNOWLEDGEMENT OF THE NOTICE OF PRIVACY PRACTICES
The KCHD Notice of Privacy Practices provides information about how we may use and disclose your protected health information.
The Notice of Privacy Practices is subject to change. To obtain a copy of our notice you may visit our website at or by
calling (304) 348-8080. By signing this form, you acknowledge that the KCHD Notice of Privacy Practices was made available to you.
CONSENT
You must be at least 18 years of age to sign. If under age 18, a parent or guardian’s signature is required. I have read or had explained
to me the 2015-2016 Vaccine Information Statement for the 2015-2015 Influenza vaccine and understand the risks and benefits. I give
consent for my child named at the top of this form to be vaccinated with this vaccine.
_____________________________________________________
_________________________________
Signature of Parent or Legal Guardian
Date
Health Department Use Only
VFC______
KCHD______
Medical Screener Signature_______________________________________________ Date_______________________________
MedImmune Intranasal
Injection
Date
Manufacturer/Vaccine:
Intranasal
------- / ------- / 2015
Influenza
Site/Route
Vaccinated:
Lot#
Place label here
Vaccinator Signature:
_________________________________
Expiration Date:
ADVERTISEMENT
0 votes
Related Articles
Related forms





 Consent Form")




Related Categories
Parent category: Legal