New York Member Enrollment Form - Ohi Page 2
ADVERTISEMENT
 1
1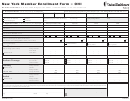 2
2New York Member Enrollment Form – OHI
MAILING ADDRESS: P. O. Box 7085, Bridgeport CT 06601 • 1-800-444-6222 • www oxfordhealth com
A. Group Information (To be completed by the employer)
Please print neatly using black or blue ballpoint pen • ALL DATES MUST BE: MM/DD/YYYY
Group Number
Group Name
Plan CSP
Billing Group
Date of Hire
Effective Date
Occupation
/
/
/
/
COBRA/Young Adult/SC Qualifying
Event Date
Employer Signature
Date
■
■
On Leave of Absence
Retired
Event
/
/
X
/
/
■
■
Union Employee
Disabled
B. Applicant Details (To be completed by the employee)
Employee/Subscriber
Spouse
Child
Child
Social Security Number:
Last Name:
First Name, Middle Initial:
Date of Birth: (MM/DD/YYYY)
/
/
/
/
/
/
/
/
■
■
■
■
■
■
■
■
■
■
■
■
Gender and Disability Status: (Check appropriate boxes.)
M
F
/
Disabled
M
F
/
Disabled
M
F
/
Disabled
M
F
/
Disabled
Primary Care Physician (PCP) ID Number:
___________________________________
__________________________________
__________________________________
___________________________________
■
■
■
■
Yes
Yes
Yes
Yes
PCP Name: ( If an
of PCP, check “Yes”. )
existing patient
■
■
Full-time Student
Full-time Student
■
Check all that apply:
Domestic Partner
■
■
Young Adult
Young Adult
Prior Carrier
Carrier:
___________________________________
___________________________________
___________________________________
___________________________________
(List coverage prior to this.)
Policy Number:
___________________________________
___________________________________
___________________________________
___________________________________
From Date
/
/
/
/
/
/
/
/
■
Same for all
Thru date::
/
/
/
/
/
/
/
/
C. Coordination of Benefits
Employee/Subscriber
Spouse
Child
Child
■
■
■
■
Check appropriate
Part A
/
/
Part A
/
/
Part A
/
/
Part A
/
/
Medicare Coverage
■
■
■
■
box and list
Part B
/
/
Part B
/
/
Part B
/
/
Part B
/
/
■
■
■
■
effective date:
Part D
/
/
Part D
/
/
Part D
/
/
Part D
/
/
Pharmacy
Policy Number:
___________________________________
___________________________________
___________________________________
___________________________________
■
Same for all
Carrier:
___________________________________
___________________________________
___________________________________
___________________________________
Policy Holder:
___________________________________
___________________________________
___________________________________
___________________________________
Effective Date:
Group Number:
BIN:
BIN:
BIN:
BIN:
/
/
PCN:
PCN:
PCN:
PCN:
Policy Number:
___________________________________
___________________________________
___________________________________
___________________________________
Medical
Carrier:
___________________________________
___________________________________
___________________________________
___________________________________
■
Same for all
Policy Holder:
___________________________________
___________________________________
___________________________________
___________________________________
Effective Date:
/
/
/
/
/
/
/
/
I
understand
that
my
enrollments
and
benefits
are
in
accordance
with
those
described
in
the
Oxford
Health
Insurance
Certificate.
I
understand
that,
in
order
to
receive
in-network
benefits,
I
and
any
enrolled
dependents
must
seek
care
through
our
Oxford
affiliated
primary
care
physician or through an Oxford-affiliated specialist physician with an authorized referral from the primary care physician if required. I further understand that if I do not adhere to these requirements, I will be eligible only for out-of-network health insurance coverage under the terms of the Certificate. Any person who knowingly and with intent to defraud any insurance company or other person files an application
for insurance or statement of claim containing any materially false information, or conceals for the purpose of misleading, information concerning any fact material thereto, commits a fraudulent insurance act, which is a crime and shall also be subject to a civil penalty not to exceed five thousand dollars and the stated value of the claim for each such violation. I authorize any health provider or insurer to furnish
Oxford any records concerning me or any enrolled member of my family for whom information is requested.
Employee’s/Young Adult’s Address (Apt #)
Employee’s/Young Adult’s Signature
Date
________________________________________________________________________________________________________
/
/
City
State
Zip
X
OHINY MEF LS 1109
4318 REV 8
ADVERTISEMENT
0 votes
Related Articles
Related forms





 - Public Employees' Retirement System Of Nevada")




Related Categories
Parent category: Medical