Provider Information Update Form Page 2
Download a blank fillable Provider Information Update Form in PDF format just by clicking the "DOWNLOAD PDF" button.
Open the file in any PDF-viewing software. Adobe Reader or any alternative for Windows or MacOS are required to access and complete fillable content.
Complete Provider Information Update Form with your personal data - all interactive fields are highlighted in places where you should type, access drop-down lists or select multiple-choice options.
Some fillable PDF-files have the option of saving the completed form that contains your own data for later use or sending it out straight away.
ADVERTISEMENT
 1
1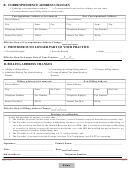 2
2B. CORRESPONDENCE ADDRESS CHANGES
□ Updating correspondence address
□ Correspondence and service address are the same
□ Correspondence and billing address are the same
Correspondence Address to be removed
New Correspondence Address
Street Address:
Street Address:
City:
State:
Zip:
City:
State:
Zip:
Telephone Number:
Fax Number:
Telephone Number:
Fax Number:
Federal Tax ID #:
NPI #:
Federal Tax ID #:
NPI #:
Effective Date of Correspondence Address Change:
/
/
C. PROVIDER IS NO LONGER PART OF YOUR PRACTICE
□
□
□
Provider Resigned
_____________
Provider Retired
Other
___/___/___
Effective Date No Longer Part of Your Practice:
D. BILLING ADDRESS CHANGES
□
□
□
Adding a billing address
Correcting an existing billing address
Closing a billing address
□
□
identification
identification
Additional Federal Tax
Closing a Federal Tax
Number
Number
Billing Address to be removed
New Billing Address
Street Address:
Street Address:
City:
State:
Zip Code:
City:
State:
Zip Code:
Telephone Number:
Fax Number:
Telephone Number:
Fax Number:
Federal Tax ID #:
NPI #:
Federal Tax ID #:
NPI #:
Effective Date of Billing Address Change:
/
/
Provider’s Certification
Under the penalties of perjury, I certify that:
1. The number of shown on this form is the Provider’s correct Federal taxpayer identification number, and
2. The Provider is not subject to backup withholding because: (a) it is exempt from backup withholding, or
(b) it has not been notified by the Internal Revenue Service (IRS) that it is subject to backup withholding
as a result of a failure to report all interest or dividends, or (c) the IRS has notified the payee that it is no
longer subject to backup withholding, and
3. The Provider is a U.S. person (including a U.S. resident alien), and
4. The Provider is exempt from the Foreign Account Tax Compliance Act (FATCA) reporting
Signature: ____________________________ Printed Name: _____________________________________
Title: ________________________________ Date:
/
/
Email address: _______________________________ Telephone Number:___________________________
Page 2
January 2016
Print
ADVERTISEMENT
0 votes
Related Articles
Related forms










Related Categories
Parent category: Business