Form 4319 - Driver Condition Report Page 2
Download a blank fillable Form 4319 - Driver Condition Report in PDF format just by clicking the "DOWNLOAD PDF" button.
Open the file in any PDF-viewing software. Adobe Reader or any alternative for Windows or MacOS are required to access and complete fillable content.
Complete Form 4319 - Driver Condition Report with your personal data - all interactive fields are highlighted in places where you should type, access drop-down lists or select multiple-choice options.
Some fillable PDF-files have the option of saving the completed form that contains your own data for later use or sending it out straight away.
ADVERTISEMENT
 1
1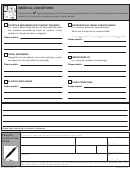 2
2MEDICAL CONDITIONS
Please check
appropriate boxes if the driver being reported has any of the following conditions that would
impair his or her ability to safely operate a motor vehicle:
COGNITIVE IMPAIRMENTS/PSYCHIATRIC DISORDER
DISORDERS THAT IMPAIR CONSCIOUSNESS
(i.e., sees or hears things that are not there, gets lost easily,
(i.e., seizures, blackouts, sleep disorders)
has problems remembering words for common things,
When was the last loss of consciousness?
confusion in thought process or judgment)
_______________/ ______________/ ______________
Please explain:
(month)
(day)
(year)
Please explain:
VISUAL IMPAIRMENT
(frequently runs into objects, cannot see road signs, cannot
LIMITED MOBILITY
see objects on the side without turning head)
(i.e., paralysis, problems moving freely)
Please explain:
Please explain:
ALCOHOL/DRUG ABUSE
OTHER CONDITIONS
Please explain:
Please explain:
ADDITIONAL COMMENTS
Please attach additional comments if necessary.
Based on my observation(s) of the above named person and/or information relayed to me by the individual, I reasonably and
PERSON
in good faith, believe that he/she cannot safely operate a motor vehicle.
COMPLETING
PRINT FULL NAME (LAST, FIRST, MIDDLE)
RELATIONSHIP TO DRIVER
TELEPHONE NUMBER
FORM:
(_ _ _) _ _ _ - _ _ _ _
STREET ADDRESS
CITY
STATE
ZIP CODE
__ __ __ __ __
SIGNATURE
DATE
_ _ / _ _ / _ _ _ _
ANY PERSON WHO INTENTIONALLY FILES A FALSE REPORT SHALL BE GUILTY OF A CLASS A MISDEMEANOR, AND
SHALL BE LIABLE FOR THE DAMAGES WHICH RESULT.
MO 860-2507 (04-2010)
DOR-4319 (04-2010)
ADVERTISEMENT
0 votes
Related Articles
Related forms










Related Categories
Parent category: Financial