Initial Credit/closed End Monthly Outstanding Balance Disability Claim Form Page 3
Download a blank fillable Initial Credit/closed End Monthly Outstanding Balance Disability Claim Form in PDF format just by clicking the "DOWNLOAD PDF" button.
Open the file in any PDF-viewing software. Adobe Reader or any alternative for Windows or MacOS are required to access and complete fillable content.
Complete Initial Credit/closed End Monthly Outstanding Balance Disability Claim Form with your personal data - all interactive fields are highlighted in places where you should type, access drop-down lists or select multiple-choice options.
Some fillable PDF-files have the option of saving the completed form that contains your own data for later use or sending it out straight away.
ADVERTISEMENT
 1
1 2
2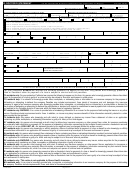 3
3 4
4D. DOCTOR’S STATEMENT
(TO BE FURNISHED WITHOUT EXPENSE TO THE INSURANCE COMPANY)
PLEASE PRINT
PATIENT’S FULL NAME
DIAGNOSIS (CODE(S))
ICD-9
CPT
DSM III
CURRENT DIAGNOSIS
LIST THE NAMES OF ALL PRESCRIBED MEDICATIONS FOR THIS DIAGNOSIS
GIVE EXACT DATES OF TOTAL DISABILITY (UNABLE TO WORK)
GIVE EXACT DATES OF PARTIAL DISABILITY
His/Her Occupation
His/Her Occupation
/
/
/
/
/
/
/
/
FROM
TO
FROM
TO
Any Occupation
Any Occupation
IN YOUR EXPERT OPINION, HOW WOULD YOU QUALIFY THIS PATIENT
IF TEMPORARILY DISABLED, HOW MUCH LONGER DO YOU EXPECT THE PATIENT TO BE DISABLED
Permanently Disabled
Temporarily Disabled
Non-Disabled
1-2 months
3 months
6 months
Longer than 9 months
Undetermined
PHYSICAL IMPAIRMENTS (AS DEFINED IN FEDERAL DICTIONARY OF OCCUPATIONAL TITLE)
Class 1 - No limitation of functional capacity; capable of heavy work; no restrictions. (0-10%)
Class 2 - Medium manual activity. (15-30%)
Class 3 - Slight limitation of functional capacity; capable of light work. (35-55%)
Class 4 - Moderate limitation of functional capacity; capable of clerical/administrative (sedentary) activity. (60-70%)
Class 5 - Severe limitation of functional capacity; incapable of minimum (sedentary) activity. (75-100%)
IS CONDITION DUE TO PREGNANCY
IF YES, DESCRIBE COMPLICATIONS
ESTIMATED DATE OF DELIVERY
/
/
Yes
No
WHEN DID SYMPTOMS FIRST APPEAR
WAS DISABILITY CAUSED BY AN ACCIDENT
IF YES, DATE OF ORIGINAL ACCIDENT
IF YES, DESCRIBE ACCIDENT
/
/
/
/
Yes
No
HAS PATIENT EVER HAD SAME OR SIMILAR CONDITION
GIVE DATES OF TREATMENT FOR SIMILAR CONDITION (MM/DD/YY)
Yes
No
DESCRIBE SAME OR SIMILAR CONDITION
GIVE NAMES, ADDRESSES, AND PHONE NUMBERS OF OTHER TREATING PHYSICIANS (ATTACH ADDITIONAL SHEET IF NECESSARY)
DATES OF TREATMENT
FREQUENCY OF VISITS
Weekly
Monthly
/
/
/
/
/
/
Other (specify)
FIRST VISIT
LAST VISIT
NEXT VISIT
HAS PATIENT BEEN HOSPITALIZED
NAME OF HOSPITAL
/
/
/
/
Yes
No
If yes,
FROM
THROUGH
STREET ADDRESS
CITY
STATE
ZIP CODE
TELEPHONE NUMBER
(
)
DATE PERFORMED
DID PATIENT HAVE SURGERY
IF YES, DESCRIBE SURGERY
/
/
Yes
No
IS PATIENT STILL UNDER YOUR CARE FOR THIS CONDITION
IF PATIENT IS STILL UNDER YOUR CARE,
IF NOT, GIVE DATE PATIENT WAS RELEASED TO RESUME WORK
GIVE ESTIMATED DATE WHEN
/
/
/
/
Yes
No
PATIENT WILL RESUME WORK
PROGNOSIS/COMMENTS (HAS PATIENT PROGRESSED)
“I hereby certify that the above described information is based upon reasonable medical probability, and is true and correct to the best of my knowledge and belief.”
STREET ADDRESS
CITY
STATE
ZIP CODE
TELEPHONE NUMBER
FAX NUMBER
(
)
(
)
ATTENDING PHYSICIAN’S NAME (PLEASE PRINT)
ATTENDING PHYSICIAN’S SIGNATURE
MEDICAL ID NUMBER
DEGREE
DATE
/
/
X
FORM MUST BE FULLY COMPLETED AND SIGNED OR STAMPED BY DOCTOR’S OFFICE
For your protection Arizona law requires the following statement to appear on this form. Any person who knowingly presents a
false or fraudulent claim for payment of a loss is subject to criminal and civil penalties
.
CA residents only: For your protection California law requires the following to appear on this form: Any person who knowingly presents a false or fraudulent
claim for the payment of a loss is guilty of a crime and may be subject to fines and confinement in state prison.
CO residents only: It is unlawful to knowingly provide false, incomplete, or misleading facts or information to an insurance company for the purpose of
defrauding or attempting to defraud the company. Penalties may include imprisonment, fines, denial of insurance, and civil damages. Any insurance
company or agent of an insurance company who knowingly provides false, incomplete, or misleading facts or information to a policyholder or claimant for
the purpose of defrauding or attempting to defraud the policyholder or claimant with regard to a settlement or award payable from insurance proceeds shall
be reported to the Colorado division of insurance within the department of regulatory agencies.
DC residents only: WARNING: It is a crime to provide false or misleading information to an insurer for the purpose of defrauding the insurer or any other
person. Penalties include imprisonment and/or fines. In addition, an insurer may deny insurance benefits if false information materially related to a claim
was provided by the applicant.
FL residents only: Any person who knowingly and with intent to injure, defraud, or deceive any insurer files a statement of claim or an application
containing any false, incomplete, or misleading information is guilty of a felony of the third degree.
KY residents only: Any person who knowingly and with intent to defraud any insurance company, or other person files a claim for insurance containing
any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance
act, which is a crime. HIGH LIMIT AD - No statements made by the applicant may be changed without his written consent.
MD residents only: Any person who knowingly or willfully presents a false or fraudulent claim for payment of a loss or benefit or who knowingly or willfully
presents false information in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison.
NJ residents only: Any person who knowingly files a statement of claim containing any false or misleading information is subject to criminal and civil penalties.
NM residents only: Any person who knowingly presents a false or fraudulent claim for payment of a loss or benefit or knowingly presents false information
in an application for insurance is guilty of a crime and may be subject to civil fines and criminal penalties.
OK residents only: WARNING: Any person who knowingly, and with intent to injure, defraud or deceive any insurer, makes any claim for the proceeds of
an insurance policy containing any false, incomplete or misleading information is guilty of a felony.
PA residents only: Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or
statement of claim containing any materially false information or conceals for the purpose of misleading, information concerning any fact material thereto
commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties.
RI residents only: Any person who knowingly presents a false or fraudulent claim for payment of a loss or benefit or knowingly presents false information
in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison.
TX residents only: Any person who knowingly presents a false or fraudulent claim for the payment of a loss is guilty of a crime and may be subject to fines
and confinement in state prison.
VA residents only: *This notice is not applicable to life and health insurance.
WA residents only: It is a crime to knowingly provide false, incomplete, or misleading information to an insurance company for the purpose of defrauding
the company. Penalties include imprisonment, fines, and denial of insurance benefits.
C1030-0412
Page 3 of 4
ADVERTISEMENT
0 votes
Related Articles
Related forms
")









Related Categories
Parent category: Legal