Form Mv-664.1 - Application For License Plates Or Parking Permits For Persons With Severe Disabilities Page 3
ADVERTISEMENT
 1
1 2
2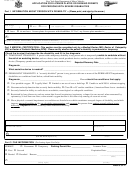 3
3 4
4New York State Department of Motor Vehicles
MV-664.1 (1/00)
APPLICATION FOR LICENSE PLATES OR PARKING PERMITS
FOR PERSONS WITH SEVERE DISABILITIES
Part 1 INFORMATION ABOUT PERSON WITH DISABILITY
—(Please print, and sign by the arrow.)
Last Name
First
M.I.
Telephone No.
(
)
Address: No. and Street
Apt. No.
City
State
Zip Code
Date of Birth
!
!
!
!
I am applying for:
License Plates
Parking Permit
Male
Female
/
/
!
!
I
have
do not have license plates for persons with disabilities. If “Yes”, my license plate number is:__________________
(Signature of Person with Disability or Signature of Parent or Guardian) —
If signed by parent or guardian,
(Date)
please state your relationship to the person with the disability after your signature.
Part 2 MEDICAL CERTIFICATION—
This section must be completed only by a Medical Doctor (MD), Doctor of Osteopathy
(DO) or Doctor of Podiatric Medicine (DPM) . Please certify whether the patient’s disability is permanent or temporary.
Check the box(es) that describe the disability, and fill in the diagnosis:
!
TEMPORARY DISABILITY: A person with a temporary disability is any person who is temporarily unable to ambulate without
the aid of an assisting device, such as a brace, cane, crutch, prosthetic device, another person, wheelchair, walker or other assistive
device. (Temporary permits are issued for periods of six months or less.)
/
/
_______________________
Expected Recovery Date
Diagnosis:_____________________________________________________________________________________________
What assistive device is needed? __________________________________________________________________________
!
PERMANENT DISABILITY: A “severely disabled” person is any person with one or more of the PERMANENT impairments,
disabilities or conditions listed below, which limit mobility.
Diagnosis:____________________________________________________ Please check the conditions that apply:
!
!
!
!
Uses portable oxygen
Legally blind
Limited or no use of one or both legs
Unable to walk 200 ft. without stopping
!
!
Neuromuscular dysfunction that severely limits mobility
Class III or IV cardiac condition. (American Heart Assoc. standards)
!
Severely limited in ability to walk due to an arthritic, neurological or orthopedic condition
!
Restricted by lung disease to such an extent that forced (respiratory) expiratory volume for one second, when measured by
spirometry, is less than one liter, or the arterial oxygen tension is less than sixty mm/hg of room air at rest
!
Has a physical or mental impairment or condition not listed above which constitutes an equal degree of disability, and which
imposes unusual hardship in the use of public transportation and prevents the person from getting around without great
difficulty. Explain how this disability limits functional mobility.
______________________________________________________________________________________________________
______________________________________________________________________________________________________
MD/DO/DPM Name
Professional License No.
Telephone No.
MD/DO/DPM Address
(
)
(MD/DO/DPM Signature)
(Date)
Part 3 FILE INFORMATION
(For Issuing Agent Use Only):
!
!
Parking Permit No. _______________
PERMIT:
Permanent
Temporary
Issuance Date: ________________
!
!
First
Second
Expiration Date: ________________
!
!
Denied
Revoked Reason:_____________________________________________________
______________________
(Date)
___________________________________________________________________________________
____________________________________________
(Issuing Agent)
(Locality)
_____________________________________________
PAGE 3 OF 4
ADVERTISEMENT
0 votes
Related Articles
Related forms
 Form-664.1 - Application For A Parking Permit Or License Plates For Persons With Severe Disabilities
Legal
Form-664.1 - Application For A Parking Permit Or License Plates For Persons With Severe Disabilities
Legal
") Form Mv-664.1ch - Application For A Parking Permit Or License Plates, For People With Severe Disabilities (chinese)
Legal
Form Mv-664.1ch - Application For A Parking Permit Or License Plates, For People With Severe Disabilities (chinese)
Legal
") Form Mv-664.1i - Application For A Parking Permit Or License Plates, For People With Severe Disabilities (italian)
Legal
Form Mv-664.1i - Application For A Parking Permit Or License Plates, For People With Severe Disabilities (italian)
Legal
") Form Mv-664.1r - Application For A Parking Permit Or License Plates, For People With Severe Disabilities (russian)
Legal
Form Mv-664.1r - Application For A Parking Permit Or License Plates, For People With Severe Disabilities (russian)
Legal
") Form Mv-664.1fc - Application For A Parking Permit Or License Plates, For People With Severe Disabilities (haitian Creole)
Legal
Form Mv-664.1fc - Application For A Parking Permit Or License Plates, For People With Severe Disabilities (haitian Creole)
Legal
") Form Mv-664.1k - Application For A Parking Permit Or License Plates, For People With Severe Disabilities (korean)
Legal
Form Mv-664.1k - Application For A Parking Permit Or License Plates, For People With Severe Disabilities (korean)
Legal
") Form Mv-664.1s - Application For A Parking Permit Or License Plates, For People With Severe Disabilities (spanish)
Legal
Form Mv-664.1s - Application For A Parking Permit Or License Plates, For People With Severe Disabilities (spanish)
Legal
 Form Mv-664.1mp - Application For A Metered Parking Waiver For Person With Severe Disabilities
Legal
Form Mv-664.1mp - Application For A Metered Parking Waiver For Person With Severe Disabilities
Legal


Related Categories
Parent category: Legal