Directions For Completing Medical Requirement Forms Page 6
ADVERTISEMENT
 1
1 2
2 3
3 4
4 5
5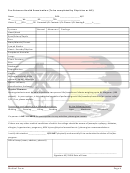 6
6 7
7 8
8Pre-Entrance Health Examination (To be completed by Physician or NP)
Name: _____________________________________ DOB: __________________ M/F
Ht: __________ Wt: __________ BP: ___________TPR: _____________________
Vision: R_____/20 L ______/20 Corrected Y/N Contacts: Y/N Glasses: Y/N Hearing R: ______ L:______
Systems
Normal Abnormal Findings
Head/Neck
Eyes/Sclera/Pupils
Ears
Nose/Mouth/Throat
Lymph Nodes
Heart: Sounds/Rhythm
Peripheral Vascular
Lungs
Chest Contour
Skin
Abdomen
Reproductive
Hernia
Musculoskeletal: ROM,
posture, spine, strength
Neuro: reflexes,
coordination, balance
Physical Clearance
Nursing students must be able to perform two person lifts/transfers of clients weighing up to 86 kilograms (190
pounds). In your opinion, is this individual capable of performing such lifts/transfers/restraints/or carries safely?
Y/N. If no, please explain: ______________________________________________________________
Person may participate in the following activities:
At the following Level:
Walking _____ Running ____ Lifting ____ Bending _____
Light _____ Moderate _____ Strenuous ___
If a person is NOT CLEARED for participation in any activities, please give reason:
_____________________________________________________________________________________
If there are any other medical conditions of which the college should be aware of (example: epilepsy, diabetes,
allergies, hypertension, pregnancy, MSK injures/physical anomalies etc.) please give recommendations:
__________________________________________________________________________________________
I certify this student _______________ IS/IS NOT physically and mentally fit to undertake the duties of his/her
program.
Office Stamp (name, address, phone #)
____________________________________________________
Signature NP/ DR & Date of Exam
Medical Form
Page 6
ADVERTISEMENT
0 votes
Related Articles
Related forms
 Form Rev-20 As - Employer Withholding For Pennsylvania Taxable Compensation Guide - Directions For Completing Federal Form W-2 Block 16
Financial
Form Rev-20 As - Employer Withholding For Pennsylvania Taxable Compensation Guide - Directions For Completing Federal Form W-2 Block 16
Financial


 Form Pa-1000 - Instructions For Completing Your Claim Form - Property Tax Or Rent Rebate Program
Financial
Form Pa-1000 - Instructions For Completing Your Claim Form - Property Tax Or Rent Rebate Program
Financial


 Cancellation Requirements - 2017, Form Llc-4/8 - Instructions For Completing The Short Form Cancellation Certificate - 2017")
")


Related Categories
Parent category: Legal