Form Gr-67834-20 - Aetna Enrollment Change Request Form Page 2
Download a blank fillable Form Gr-67834-20 - Aetna Enrollment Change Request Form in PDF format just by clicking the "DOWNLOAD PDF" button.
Open the file in any PDF-viewing software. Adobe Reader or any alternative for Windows or MacOS are required to access and complete fillable content.
Complete Form Gr-67834-20 - Aetna Enrollment Change Request Form with your personal data - all interactive fields are highlighted in places where you should type, access drop-down lists or select multiple-choice options.
Some fillable PDF-files have the option of saving the completed form that contains your own data for later use or sending it out straight away.
ADVERTISEMENT
 1
1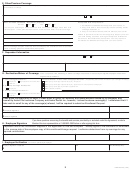 2
2 3
3E. Other/Previous Coverage
If you have checked "Yes" to Other Dental Coverage (Section C), provide name(s) and policy number(s) of insurance carrier(s), dental plan, or other source; a copy of the insurance card(s), and
the start date(s) of coverage.
Is your Spouse/Civil Union Partner employed? If Yes, provide name and address of spouse's/civil union partner's employer.
Yes
No
PROOF OF PRIOR COVERAGE - IMPORTANT (Required)
Acceptable forms of proof are:
Dental:
Life:
Yes
No
Yes
No
1. Certificate of Creditable Coverage from prior carrier, or
Does anyone enrolling on this enrollment form have prior coverage other than with
2. Copy of ID card or most recent payroll stub showing dental
this employer? If Yes, provide their names, start and end dates of prior coverage.
coverage deduction, or
3. Copy of most recent dental premium bill from prior carrier.
Failure to provide Proof of Prior Coverage may subject you to the
12 month waiting period for coverage of Major and Orthodontic
Services on the Dental PPO plan options. You may request a
Certificate of Creditable Coverage from your prior carrier.
Proof of coverage and plan summary must accompany this enrollment form for possible
waiver of waiting period on Dental PPO plan options.
F. Dependent Information
Does any dependent listed in Section D live at a different address than the Employee? If "Yes," who and what address?
Yes
No
Explain the circumstances.
If any dependent's last name differs from yours, explain the circumstances.
G. Declination/Waiver of Coverage
- To be completed if life, disability, or dental coverage is declined or refused by an eligible employee and/or their
eligible family members.
1. Life Coverage Declined for:
Reason for Refusal - Please check all appropriate boxes.
(If applicable, please attach front/back of your coverage ID card(s).)
Employee
Spouse/Civil Union Partner
Other group coverage sponsored by my employer.
Children
Other group coverage sponsored by my spouse's/civil union partner's employer.
2. Disability Coverage Declined for:
Other group coverage by another organization.
Employee
Other (please explain):
3. Dental Coverage Declined for:
Please provide name of carrier and policy number.
Employee
Spouse/Civil Union Partner
Children
I was given the opportunity to enroll in these plans of group life, disability, and dental benefits offered by my employer and
insured by Aetna Life Insurance Company and Aetna Dental Inc.; however, I refuse the above coverage(s). I understand that if I
later wish to enroll for any of the coverage(s) refused, I will be required to submit an Enrollment
Request.
Please sign here ONLY if you are declining coverage for yourself or dependent(s).
Date (Month/Day/Year)
X
Employee Signature
Date (Month/Day/Year)
X
Witness Signature
If you have questions concerning the benefits and services provided by or excluded under this Agreement, contact a
H. Employee Signature
Member Services representative at 1-888-802-3862 before or after signing this form.
I represent that all the information supplied in this application is true and complete. I hereby agree to the conditions of enrollment
on the reverse side of the employee copy of this enrollment/change request. I authorize deductions from my earnings for any
required contributions.
Employee Signature - Required
E-Mail Address
Date (Month/Day/Year)
X
I. Employer Verification
- To Be Completed by Employer
Employer Signature - Required
Title
Date (Month/Day/Year)
X
2
GR-67834-20 (7-08)
ADVERTISEMENT
0 votes
Related Articles
Related forms










Related Categories
Parent category: Business