Family, Social And Occupational Health History Page 2
ADVERTISEMENT
 1
1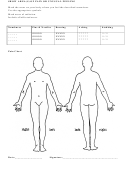 2
2SHOW AREA(S) OF PAIN OR UNUSUAL FEELING
Mark the areas on your body where you feel the described sensations.
Use the appropriate symbols.
Mark areas of radiation.
Include all affected areas.
Numbness
Pins & Needles
Burning
Aching
Stabbing
_ _ _ _ _
OOOOO
XXXXX
* * * * *
/ / / / /
_ _ _ _ _
OOOOO
XXXXX
* * * * *
/ / / / /
_ _ _ _ _
OOOOO
XXXXX
* * * * *
/ / / / /
Pain Chart
Date:___________________
Signature:______________________________________
ADVERTISEMENT
0 votes
Related Articles
Related forms










Related Categories
Parent category: Medical