Complete Name of Insured
a. Policy Number
b. Coverage Start Date
c. Coverage Expiration
d. Date Premium Due/Paid
e. Full Name of Non-admitted Insurer or Lloyd's Broker/Syndicate
f. Insurer's or Lloyd's Broker Address
City
State
Country
ZIP Code
g. Type of Insurance
h. Property/Risk Covered by the Insurance
i.
j. % of property/risk w/in AZ
k. AZ PREMIUM AMOUNT
X
FULL PREMIUM AMOUNT
F4
=
%
$0.00
l. Which criteria did you use to allocate Arizona's portion of multistate premium (check all that apply):
100% AZ - not applicable
Physical assets
Employee payroll
Sales
Taxable income
Other (describe): __________________________________________________________________________
m. Total full-time employees or equivalents as of the date the policy was issued by the
unauthorized insurer:
n. If "F1k" was less than 80, the total full-time or equivalent employees of the insured's holding
company system as of the policy issuance date:
a. Policy Number
b. Coverage Start Date
c. Coverage Expiration
d. Date Premium Due/Paid
e. Full Name of Non-admitted Insurer or Lloyd's Broker/Syndicate
f. Insurer's or Lloyd's Broker Address
City
State
Country
ZIP Code
g. Type of Insurance
h. Property/Risk Covered by the Insurance
i.
j. % of property/risk w/in AZ
k. AZ PREMIUM AMOUNT
FULL PREMIUM AMOUNT
X
F5
=
%
$0.00
l. Which criteria did you use to allocate Arizona's portion of multistate premium (check all that apply):
100% AZ - not applicable
Physical assets
Employee payroll
Sales
Taxable income
Other (describe): __________________________________________________________________________
m. Total full-time employees or equivalents as of the date the policy was issued by the
unauthorized insurer:
n. If "F1k" was less than 80, the total full-time or equivalent employees of the insured's holding
company system as of the policy issuance date:
If you procured more than 5 insurance policies from unauthorized insurers, attach additional signed and dated
pages containing the same information requested for each of the foregoing policies and attach a signed and dated
sheet showing the calculation in F6 for all the policies you report.
Line
[a] - FULL PREMIUM AMOUNT
[b] - % w/in AZ
[c] = [a] x [b]
%
$0.00
0.00
$0.00
F1
%
$0.00
0.00
$0.00
F2
%
$0.00
0.00
$0.00
F3
%
$0.00
0.00
$0.00
F6
F4
%
$0.00
0.00
$0.00
F5
$0.00
$0.00
COLUMN
F6c: Post Total of [c] to
TOTALS
Section B, Line B1
SECTION G: CERTIFICATION OF INDUSTRIAL INSURED
By my signature, I hereby certify that I am authorized to act for the Insured, that all the information contained in
this report has been verified, and that all the information in this report is true, correct and complete.
Signature
Date
__________________________________________________________
Printed Name
Title
Industrial Insureds Premium Receipts Report
Page 5 of 5
Form E-IndIns (v20111027)
 1
1 2
2 3
3 4
4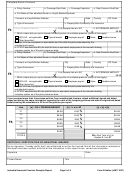 5
5
 Form It-40pnr - Schedule Ct-40pnr - County Tax Schedule For Part-year And Full-year Indiana Nonresidents - 2011
Financial
Form It-40pnr - Schedule Ct-40pnr - County Tax Schedule For Part-year And Full-year Indiana Nonresidents - 2011
Financial
 - 2011") Form It-141 - West Virginia Fiduciary Income Tax Return (for Resident And Non-resident Estates And Trusts) - 2011
Financial
Form It-141 - West Virginia Fiduciary Income Tax Return (for Resident And Non-resident Estates And Trusts) - 2011
Financial






