Dd Form 2876 - Tricare Prime Enrollment, Disenrollment, And Primary Care Manager (Pcm) Page 4
Download a blank fillable Dd Form 2876 - Tricare Prime Enrollment, Disenrollment, And Primary Care Manager (Pcm) in PDF format just by clicking the "DOWNLOAD PDF" button.
Open the file in any PDF-viewing software. Adobe Reader or any alternative for Windows or MacOS are required to access and complete fillable content.
Complete Dd Form 2876 - Tricare Prime Enrollment, Disenrollment, And Primary Care Manager (Pcm) with your personal data - all interactive fields are highlighted in places where you should type, access drop-down lists or select multiple-choice options.
Some fillable PDF-files have the option of saving the completed form that contains your own data for later use or sending it out straight away.
ADVERTISEMENT
 Printable pdf") 1
1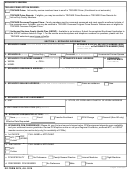 2
2 3
3 4
4 5
5SPONSOR'S SSN/DBN:
SECTION III - REASON FOR DISENROLLMENT OR PCM CHANGE
SECTION III - REASON FOR DISENROLLMENT OR PCM CHANGE
(Complete if disenrolling or making a PCM change)
Name of Family Member:
Relocation
Dissatisfied
PCS
Other:
Name of Family Member:
Relocation
Dissatisfied
PCS
Other:
Name of Family Member:
Relocation
Dissatisfied
PCS
Other:
Name of Family Member:
Relocation
Dissatisfied
PCS
Other:
SECTION IV - OTHER HEALTH INSURANCE
PLEASE IDENTIFY IF ANYONE IS CURRENTLY COVERED BY OTHER HEALTH INSURANCE.
TRICARE Supplement
(no other information is needed)
Medical Insurance:
Person(s) Covered:
Policy Holder Name:
Carrier Name:
Policy Number:
Policy Effective Date:
Dental Insurance:
Person(s) Covered:
Policy Holder Name:
Carrier Name:
Policy Number:
Policy Effective Date:
Vision Insurance:
Person(s) Covered:
Policy Holder Name:
Carrier Name:
Policy Number:
Policy Effective Date:
Prescription Insurance:
Person(s) Covered:
Policy Holder Name:
Carrier Name:
Policy Number:
Policy Effective Date:
SECTION V - ACCESS WAIVER AND SIGNATURE (REQUIRED)
If my selected or assigned Primary Care Manager (PCM) is greater than a 30 minute drive-time from my
(X if waiving drive time)
residence, or if I reside outside the Prime Service Area, I hereby waive the drive time standards of thirty minutes for primary care and
one hour for specialty care
I understand if I selected a PCM by name, team, or location (MTF or civilian), TRICARE will enroll me with that PCM subject to PCM
availability and uniformed services policy. I understand that it is my responsibility to comply with all TRICARE Prime, TRICARE Prime
Remote, TRICARE Overseas Program Prime, and/or USFHP policies and procedures. By signing this form, I certify the information
provided is true, accurate and complete. Federal funds are involved in this program and any false claims, statements, comments, or
concealment of a material fact may be subject to fine and/or imprisonment under applicable Federal law.
1. SIGNATURE OF SPONSOR, SPOUSE, OR OTHER
2. RELATIONSHIP TO SPONSOR
3. DATE SIGNED
(YYYYMMDD)
LEGAL GUARDIAN OF BENEFICIARY
ENROLLMENT NOTE: Prime enrollment start dates are based primarily on the 20th of the month rule (applications received on/before the
20th of the month are effective the first calendar day of the next month). You should confirm enrollment and PCM assignment before
obtaining routine medical care. (Note: This does not apply to TRICARE Overseas Prime or to active duty service members.)
DISENROLLMENT NOTE: In some cases, you may not be able to re-enroll in TRICARE Prime for a 12-month period from the date of the
disenrollment. This one year period does not apply to any family member whose sponsor is in grade E-1 to E-4.
PAYMENT OPTIONS: See Section VI on next page.
DD FORM 2876, JUL 2016
Page 4 of 5 Pages
ADVERTISEMENT
0 votes
Related Articles
Related forms
")
 Change")








Related Categories
Parent category: Business