Case Report Form - U.s. Department Of Health And Human Services Page 3
ADVERTISEMENT
 1
1 2
2 3
3 4
4 5
5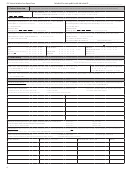 6
6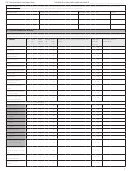 7
7 8
8 9
9 10
10 11
11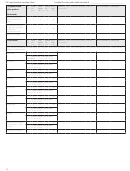 12
12 13
13CDC Listeria Initiative Case Report Form
PulseNet ID or state public health lab isolate ID ____________________________
State epi case ID ___________________
Local epi case ID ____________________
Date form completed:
/
/
FoodNet ID (if applicable) _______________________________
NNDSS ID (if available) ___ ___ ___ ___ ___
Name of interviewer
first name
last name
Was the isolate sent to public health laboratory? £ Yes £ No £ Unknown
If No, why not, and could it still be obtained? ________________________
BOX 1: Case-patient demographic data
State of residence ___ ___
County _______________
Age _____ (if pregnancy-associated, use age of mother)
Sex £ Male £ Female £ Unknown
Ethnicity: Is the case-patient of Hispanic, Latino, or Spanish origin? (one or more categories may be selected)
£ Yes ----------------------------------------------------> If yes:
£ Mexican, Mexican American, Chicano
£ Another Hispanic, Latino, or Spanish origin (specify)
£ No
£ Puerto Rican
______________________
£ Unknown
£ Cuban
£ Unknown Hispanic ancestry/declined to specify
£ Declined to answer
Race (One or more categories may be selected)
£ African American/Black
£ Asian (specify)
£ White (specify)
£ Asian Indian
£ Middle Eastern/North African
£ Native American Indian or Alaska Native
£ Chinese
£ Not Middle Eastern/North African
£ Native Hawaiian or other Pacific Islander (specify)
£ Filipino
£ Unknown
£ Native Hawaiian
£ Japanese
£ Guamanian or Chamorro
£ Other (specify) _____________________
£ Korean
£ Samoan
£ Vietnamese
£ Declined to answer
£ Other Pacific Islander
£ Other Asian (specify) _________________
BOX 2: Is the Listeria case associated with pregnancy? (Illness in pregnant woman, fetus, or infants ≤60 days old)
£ Yes If yes, skip to Box 4.
£ No
£ Unknown
BOX 3: Cases not associated with pregnancy (Illness in non-pregnant adults and children >60 days old)
Type(s) of specimen(s) that grew Listeria
Specimen collection date
State public health lab isolate ID #
(check all that apply)
(mm/dd/yyyy)
(Important: must have at least one, if available)
£ Blood
____/____/____
£ CSF
____/____/____
£ Other (specify)
____/____/____
____/____/____
£ Other (specify)
Did patient have any of the following type(s) of illnesses related to the Listeria infection? (check all that apply)
£ Bloodstream infection/sepsis £ Meningitis
£ Meningoencephalitis £ Brain abscess £ Rhombencephalitis £ Peritonitis £ Pneumonia £ Wound infection
£ Joint infection/septic arthritis £ Bone infection/osteomyelitis £ Unknown £ Other (specify) _______________________________________
Was patient hospitalized for listeriosis? £ Yes £ No £ Unknown
If yes: Admit date:
/
/
Discharge date:
/
/
£ Still hospitalized as of:
/
/
Patient’s outcome: £ Survived £ Died £ Unknown
Date of death:
/
/
If died: Was listeriosis or Listeria infection listed on death certificate? £ Yes £ No £ Unknown
If survived: Last known date alive?
/
/
BOX 4: Cases associated with pregnancy (Illness in pregnant woman, fetus, or infants ≤60 days old)
Type(s) of specimen(s) that grew Listeria
Specimen collection date
State public health lab isolate ID #
(check all that apply)
(
/
/
)
(Important: must have at least one, if available)
mm
dd
yyyy
£ Blood from mother
____/____/____
£ Blood from infant
____/____/____
£ CSF from mother
____/____/____
£ CSF from infant
____/____/____
£ Placenta
____/____/____
£ Amniotic fluid
____/____/____
£ Fetal tissue
____/____/____
£ Other (specify)
____/____/____
£ Other (specify)
____/____/____
3
ADVERTISEMENT
0 votes
Related Articles
Related forms


 Healthcare Provider Office Information Form - U.s. Department Of Health And Human Services - 2015
Legal
Healthcare Provider Office Information Form - U.s. Department Of Health And Human Services - 2015
Legal
 - Academic Enrollment Certification And Service Obligation Deferment Request - U.s. Department Of Health And Human Services") Form Nih 2762-3 - Undergraduate Scholarship Program (ugsp) - Academic Enrollment Certification And Service Obligation Deferment Request - U.s. Department Of Health And Human Services
Legal
Form Nih 2762-3 - Undergraduate Scholarship Program (ugsp) - Academic Enrollment Certification And Service Obligation Deferment Request - U.s. Department Of Health And Human Services
Legal
 Form Acf-196t - Administration For Children And Families - U. S. Department Of Health And Human Services
Legal
Form Acf-196t - Administration For Children And Families - U. S. Department Of Health And Human Services
Legal
 Form Dhhs 1662 - Nursing Record Of Tuberculosis Contacts Form - U.c. Department Of Health And Human Services
Legal
Form Dhhs 1662 - Nursing Record Of Tuberculosis Contacts Form - U.c. Department Of Health And Human Services
Legal
 Form Dhsr/hcpr 4503 - Name/address Change Reporting Form - N.c. Department Of Health And Human Services
Legal
Form Dhsr/hcpr 4503 - Name/address Change Reporting Form - N.c. Department Of Health And Human Services
Legal
 Guidance For Industry And Food And Drug Administration Staff - U.s. Department Of Health And Human Services - 2012
Legal
Guidance For Industry And Food And Drug Administration Staff - U.s. Department Of Health And Human Services - 2012
Legal


Related Categories
Parent category: Legal