State Of New Hampshire Vendor Application - Nh State Parks Page 2
ADVERTISEMENT
 1
1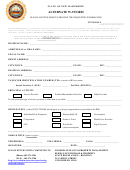 2
2STATE OF NEW HAMPSHIRE
ALTERNATE W-9 FORM
PLEASE USE THIS FORM TO PROVIDE THE REQUESTED INFORMATION
VENDOR # _________________
(Assigned by Purchase & Property)
Pursuant to IRS Regulations, you must furnish your Taxpayer Identification Number (TIN) to the State whether or not you are required to file tax returns. If this
number is not provided, you may be subject to a 28% withholding on each payment made to you. To avoid this 28% withholding & to ensure that accurate tax
information is reported to the IRS, A RESPONSE IS REQUIRED.
If a service provider is a part of a GROUP PRACTICE, it is the group name & TIN which is required on this Alternate W-9.
If the service provider is a SOLE PROPRIETOR, it is the individual name & TIN which is required on this Alternate W-9.
BUSINESS NAME: _____________________________________________________________________________
ADDITIONAL or DBA NAME: ___________________________________________________________________
LEGAL NAME: ________________________________________________________________________________
REMIT ADDRESS: _____________________________________________________________________________
CITY/TOWN: ________________________________________ STATE: _____________ ZIP: ______________
BUSINESS ADDRESS: __________________________________________________________________________
CITY/TOWN: ________________________________________ STATE: _____________ ZIP: ______________
TAXPAYER IDENTIFICATION NUMBER (TIN)
as used on IRS tax return
Social Security # (SSN): ______________________ Fed ID # (EIN/FIN): ________________________
PRINCIPAL ACTIVITY
Service Provider
Product/Merchandise Provider
Other Provider
______________________________________________
List the principal type of service, product or other that is provided:
_______________________________________________________________________________________________
DESIGNATION
(select ONLY THOSE which apply to you/your organization as provided to the IRS)
Individual/Sole-Proprietor
Partnership/LLP
Government
Corporation
Estate or Trust
Health Care Provider
LLC
Non-Profit
Legal Services
(attach exemption)
Under penalty of perjury, I declare that the information provided is true, correct & complete, to the best of my knowledge & belief.
NAME & TITLE (print or type): __________________________________________________________________
TELEPHONE #: ________________
TOLL FREE #: ________________
FAX #: _______________________
SIGNATURE: ___________________________________________ DATE: _________________________
PLEASE RETURN WHEN COMPLETED TO:
DIVISION OF PLANT & PROPERTY MANAGEMENT
BUREAU OF PURCHASE & PROPERTY
(Phone) 603-271-2201
STATE HOUSE ANNEX – ROOM 102
(FAX) 603-271-2700
25 CAPITOL STREET
CONCORD NH 03301
prchweb@nh.gov
ADVERTISEMENT
0 votes
Related Articles
Related forms

 Dissolution Legal Separation Or Annulment") State Of New Hampshire Certificate Of Divorce, Civil Union (cu) Dissolution Legal Separation Or Annulment
Business
State Of New Hampshire Certificate Of Divorce, Civil Union (cu) Dissolution Legal Separation Or Annulment
Business

") New Hampshire Housing Application For The Reissuance Of A Mortgage Credit Certificate (mcc)
Financial
New Hampshire Housing Application For The Reissuance Of A Mortgage Credit Certificate (mcc)
Financial


 Form Rt115r - Schedule Of Sales To New Hampshire Retail Dealers - Departament Of Safety Road Toll Bureau, State Of New Hampshire
Legal
Form Rt115r - Schedule Of Sales To New Hampshire Retail Dealers - Departament Of Safety Road Toll Bureau, State Of New Hampshire
Legal
 Form Dssp380 - New Hampshire Criminal History Record Information Authorization Form - Driver Education Instructions - State Of New Hampshire
Legal
Form Dssp380 - New Hampshire Criminal History Record Information Authorization Form - Driver Education Instructions - State Of New Hampshire
Legal


Related Categories
Parent category: Business