Form Tc-805 - Collection Information For Individuals - 2009 Page 3
Download a blank fillable Form Tc-805 - Collection Information For Individuals - 2009 in PDF format just by clicking the "DOWNLOAD PDF" button.
Open the file in any PDF-viewing software. Adobe Reader or any alternative for Windows or MacOS are required to access and complete fillable content.
Complete Form Tc-805 - Collection Information For Individuals - 2009 with your personal data - all interactive fields are highlighted in places where you should type, access drop-down lists or select multiple-choice options.
Some fillable PDF-files have the option of saving the completed form that contains your own data for later use or sending it out straight away.
ADVERTISEMENT
 1
1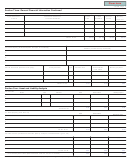 2
2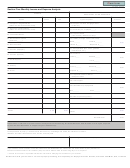 3
3Clear form
TC-805, Page 3
Section Five: Monthly Income and Expense Analysis
INCOME
NECESSARY LIVING EXPENSES
Source
Gross
Net
Type of expense
Amount
40. Rent (do not show mortgage listed
30. Taxpayer’s wages/salaries
$
$
(attach 2 most recent check stubs)
in item 27)
31. Spouse’s wages/salaries
$
41. Groceries (no. of people ____)
(attach 2 most recent check stubs)
42. Payment Totals
32. Interest/Dividends
(from line 29) "Official Use Only"
43. Utilities (average of last 12 months)
33. Net business income
(from form_____)
Gas $______
Water $_______
0.00
34. Rental income
Telephone $_____
Electric $_____
44. Transportation (bus, fares, gasoline
35. Pension (taxpayer)
maintenance, etc.)
45. Insurance
36. Pension (spouse)
Home $____
Health $_____
0.00
37. Child Support
Car $______
46. Medical
38. Alimony
Doctor $______
Dentist $_____
0.00
39. Other
Hospitals $_____
Other $______
47. Payments made to IRS for
delinquent taxes
48. Child support
49. Estimated tax prepayments
0.00
IRS ______
State ______
50. Other expenses (specify)
0.00
$
0.00
$
$
0.00
TOTAL
TOTAL
Net difference
$
0.00
Information contained in this document is subject to verification by the Utah State Tax Commission. You may be required
to provide documentation in support of your statement(s).
Under penalties of perjury, I declare that to the best of my knowledge and belief, this statement of assets,
liabilities, and other information is true, correct, and complete.
Your signature: (required)
Date
Spouses signature (required if jointly liable)
Date
If you need an accommodation under the American’s with Disabilities Act, contact the Tax Commission at (801) 297-3811 or
Telecommunications Device for the Deaf (801) 297-3819. Please allow three working days for a response.
** Failure to furnish ALL requested information will result in delaying the resolution of your account.
DO NOT mail with your tax return. To insure proper processing, mail separately to: Taxpayer Services Division, 210 North 1950 West, SLC, UT 84134
ADVERTISEMENT
0 votes
Related Articles
Related forms








")

Related Categories
Parent category: Financial