Massachusetts Department Of Transitional Assistance Food Stamp Benefits Application Page 3
ADVERTISEMENT
 1
1 2
2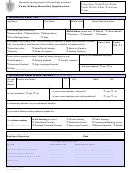 3
3 4
4 5
5 6
6 7
7 8
8Massachusetts Department of Transitional Assistance
Source:
(please check one)
Project Bread
DMH
SSA
DMR
Food Stamp Benefits Application
FEMA
CNAP
BMC
Food Pantry
Other ________________
1. Information About You
(answer all boxes)
Last Name
First Name
Middle Initial
Social Security Number
Is this name your (check one)
Marital Status (check one)
Married
Never Married
Name at Birth
Maiden Name
Married Name
Divorced
Separated
Widowed
Prior Marriage Name
Alias
Your ethnic origin (check one) This information is collected to make sure everyone is treated
Date of Birth
Gender
fairly. Your answer is voluntary and it will not affect your eligibility or benefit amount.
M
F
/
/
American Indian
Asian/Pacific Islander
Black not Hispanic
Hispanic
White not Hispanic
Alaskan American
What is your preferred language?
Do you have a special situation? (check all boxes that appy to you)
Handicapped
Hearing Impaired
Visually Impaired
Interpreter Required
Sign Language Required
Are you pregnant?
yes
no
Other________________________________________
2. Information About Where You Live
(answer all boxes)
Number and Street
Apt #
City
State
ZIP
List your
current
address
Is your current address temporary?
yes
no
Are you homeless?
yes
no
Is your current address your mailing address?
yes
no
If a temporary address, list your permanent address.
If you have a different mailing address, please list.
Is the housing you live in
Private Housing
Public Housing
Your phone number
Transitional Housing
Residential Facility
Commercial Boarding House
(____)____-_________
Employer-Provided Housing
Teen Living Program
Migrant Campsite
Shelter
______________________________________________
____/_____/___________
Applicant Signature
Date
FOR DEPARTMENT USE ONLY
ACTION
DATE COMPLETED
SIGNATURE OF STAFF
Application Received and Assigned
___/___/______
____________________________________
Information entered on BEACON
___/___/______
____________________________________
Interview Scheduled
Phone
Office
___/___/______
____________________________________
Interview Held
___/___/______
____________________________________
FSA-1 (Rev. 3/2004)
25-170-0304-05
ADVERTISEMENT
0 votes
Related Articles
Related forms


 Mail/fax Cover Sheet - Department Of Transitional Assistance (dta) Electronic Document Management") (edm) Mail/fax Cover Sheet - Department Of Transitional Assistance (dta) Electronic Document Management
Business
(edm) Mail/fax Cover Sheet - Department Of Transitional Assistance (dta) Electronic Document Management
Business

 Application For Automatic Six-month Extension - Massachusetts Department Of Revenue - 1998
Financial
Application For Automatic Six-month Extension - Massachusetts Department Of Revenue - 1998
Financial
 Massachusetts Department Of Public Health Authorization For Release Of Information Permission To Share Information
Medical
Massachusetts Department Of Public Health Authorization For Release Of Information Permission To Share Information
Medical
 Massachusetts Department Of Environmental Protection - Drinking Water Program Dbpr Tt Compliance Report
Legal
Massachusetts Department Of Environmental Protection - Drinking Water Program Dbpr Tt Compliance Report
Legal



Related Categories
Parent category: Legal