Form 323 - Quarterly Premium Tax Statement - 2004
ADVERTISEMENT
 1
1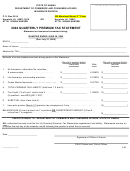 2
2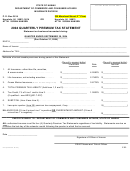 3
3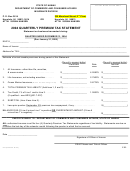 4
4DO NOT WRITE IN THIS AREA
STATE OF HAWAII
DEPARTMENT OF COMMERCE AND CONSUMER AFFAIRS
INSURANCE DIVISION
nd
P. O. Box 3614
335 Merchant Street, 2
Floor
Honolulu, HI 96811-3614
OR
Honolulu, HI 96813
ATTN: SUSAN HANSEN
ATTN: SUSAN HANSEN
2004 QUARTERLY PREMIUM TAX STATEMENT
Statement on business transacted during:
QUARTER ENDED MARCH 31, 2004
(Due April 30, 2004)
NAIC # _______________
Name of Insurer: _______________________________________________________________________________________
Address for TAX: _______________________________________________________________________________________
Estimate of actual taxable premiums during period of this Statement.
(Round to nearest dollar)
(Round to nearest dollar)
Premiums
Rate
Amount
1.
All Insurance---other than life, annuities,
& ocean marine . . . . . . . . . . . . . . . . . . . . . . . . .
$ ____________________
4.2650%
$ ____________________
2.
Life Insurance, not including annuities . . . . . . . .
$ ____________________
2.7500%
$ ____________________
3.
Ocean Marine Insurance
$ ____________________
0.8775%
$ ____________________
(Gross Underwriting Profit)
4.
TOTAL PREMIUM TAX LIABILITY (Add lines 1, 2 and 3) . . . . . . . . . . . . . . . . . . . . . . . . . .
$ ____________________
5.
Tax Credit, 1% of Line 1 and/or Line 2 . . . . . . . . .
$ ____________________
1.0000%
$ (___________________)
(If qualified – see HRS §431:7-207)
6.
SUBTOTAL (Line 4 less Line 5) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
$ ____________________
7.
Less prior year (2003) premium tax overpayment, if any . . . . . . . . . . . . . . . . . . . . . . . . . . .
$ (___________________)
BALANCE DUE (If Line 6 minus Line 7 is positive) OR OVERPAYMENT AMOUNT (If Line 6
minus Line 7 is negative) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
$ ____________________
CHECK PAYABLE TO: DEPARTMENT OF COMMERCE AND CONSUMER AFFAIRS, STATE OF HAWAII
ALL authorized insurers must file four (4) Quarterly Premium Tax Statements regardless of tax liability. Statements are due on
or before the last day of the calendar month following the quarter in which the tax accrued.
Date ________________________
Signature of Officer of Insurer
PRINT Name and Title of Officer
I01
323 (Revised 10/03)
ADVERTISEMENT
0 votes
Related Articles
Related forms










Related Categories
Parent category: Legal