Form Il-1363 - Circuit Breaker And Pharmaceutical Assistance Claim - 1999 Page 2
ADVERTISEMENT
 1
1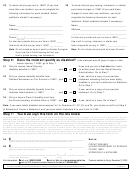 2
229
To whom did you pay rent in 1999? (If you had
30
To whom did you pay nursing, retirement, or shelter
more than one landlord, you must complete the
care home charges in 1999? (If you paid these
following information for each landlord. Attach
charges to more than one institution, you must
additional sheets if necessary.)
complete the following information for each
institution. Attach additional sheets if necessary.)
Name ___________________________________
Name ____________________________________
Address__________________________________
Address___________________________________
_________________________________________
__________________________________________
-
Phone (_____) _______________
For how many months did you live here in 1999? _______
Area code
For how many months did you rent here in 1999? _____
How much in nursing, retirement, or shelter care
How much rent did you pay here in 1999? ___________
home charges did you pay in 1999?__________________
Note: Do not include an amount paid by a Section 8 program.
Note: Do not include amounts paid by Human Services.
If you now live in Public Housing but last year
lived in private housing, see instructions.
Step 6: Does the claimant qualify as disabled?
If the claimant was 65 years of age or older
before January 1, 2000, go to Step 7.
31
Did you receive Social Security
If yes and you are a first-time filer, send
disability benefits in 1999? . . . . . . . . . . . . . . yes
no
us written proof from the Social Security
Administration. Go to Step 7.
32
Did you receive disability benefits from
If yes, send us a copy of your pension
Railroad Retirement or Civil Service in 1999? . yes
no
statement indicating that you were totally
disabled or you had a deduction for Medicare.
Go to Step 7.
33
Did you receive disability benefits from the
If yes, send us a copy of your pension
Veterans Administration in 1999? . . . . . . . . . yes
no
statement. Go to Step 7.
34
Did you have a Class 2 disability card from
the Illinois secretary of state’s office in 1999?. . yes
no
If yes, send us a copy. Go to Step 7.
Note: If you were totally disabled and answered “no” to Questions 31, 32, 33, and 34, your doctor must fill out Step 2
of Schedule A, Doctor’s Statement, and you must attach Schedule A to your Form IL-1363.
Step 7: You must sign this form on the line below
Under penalties of perjury, I state that I have examined this form and, to the best of my knowledge, it is true, correct, and complete. I give the
Illinois Department of Revenue permission to get records from anyone, including the Social Security Administration, concerning information I
have placed on this form. This consent includes my authorization for the Social Security Administration to release my Social Security number,
name, date of birth, and payment amounts for calendar years 1999 and 2000 for Circuit Breaker and Pharmaceutical Assistance claim
processing. This consent is in effect until such time as I withdraw my authorization. I also hereby assign to the Illinois Department of Revenue
my right to any benefits, including reimbursement, under any insurance plan or from any liable third party, for prescription drugs that I receive
through the Pharmaceutical Assistance program. I also agree that if I receive any such payments in error, I will repay them to the Illinois
Department of Revenue. I authorize exchange of health care information between any drug utilization review service authorized by the
department and any of my physicians and pharmacists to the extent necessary for the operation of a drug utilization review service.
X
35
___________________________________________________
Mail to:
Claimant’s signature (If you are able only to make a mark, someone else must sign as witness.) Date
CIRCUIT BREAKER
X
36
___________________________________________________
ILLINOIS DEPARTMENT OF REVENUE
PO BOX 19003
Claimant’s husband’s or wife’s signature (If filing together)
Date
SPRINGFIELD IL 62794-9003
-
________________________________ (_____) ____________
Preparer’s name (Print or type.)
Date
Phone
For information,
call us at 1 800 624-2459
visit our Web site at
Postmark deadline for filing is December 31, 2000.
call our TDD (telecommunications device for the deaf) at 1 800 544-5304
This form is authorized as outlined by the Senior Citizens and Disabled Persons Property Tax Relief and Pharmaceutical Assistance Act. Disclosure of this information is REQUIRED. Failure to provide
information could delay your grant and/or pharmaceutical coverage. This form has been approved by the Forms Management Center.
IL-492-2740
IL-1363 back (R-12/99)
ADVERTISEMENT
0 votes
Related Articles
Related forms










Related Categories
Parent category: Financial