Form 382-A - Application For Reimbursement Of Expenses Page 3
ADVERTISEMENT
 1
1 2
2 3
3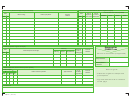 4
4APPLICATION FOR REIMBURSEMENT OF EXPENSES
Occupational health and safety
For worker
For person accompanying the worker
Other
1. Information about the person applying for reimbursement
2. Information about worker
Surname (as shown on birth certificate) and first name
Telephone
Worker’s file No.
Home Adress, Number, Street, Apt.
Date of original event
Y Y Y Y
M M
D D
City, Province, Country
Date of recurrence,
Postal code
Y Y Y Y
M M
D D
relapse or aggravation
3. Travel Expenses (attach original receipts)
Date
Amount Claimed
Reason for travel
Distance
Method of
To
From
of round
transportation used
Physio
Occ.
Transpor-
Parking
Other (Specify)
trip (km)
Month
Day
Therapy
(√)
tation
and tolls
(√)
If the worker must be accompanied, attach the medical prescription to that effect and indicate:
Surname (as shown on birth certificate) and first name of person accompanying the worker
Telephone
Advance received
$
(if applicable)
Home Adress, Number, Street, Apt.
City, Province, Country
Signature of person
Y Y Y Y
M M
D D
applying for reimbursement
Detach and return to the CNESST
3 8 2 - A
(2017-07)
ADVERTISEMENT
0 votes
Related Articles
Related forms

 Form 1127-a - Application For Extension Of Time For Payment Of Income Tax For 2011 Due To Undue Hardship - 2011
Financial
Form 1127-a - Application For Extension Of Time For Payment Of Income Tax For 2011 Due To Undue Hardship - 2011
Financial
 Form 5434-a - Application For Renewal Of Enrollment - Joint Board For The Enrollment Of Actuaries - 2017
Financial
Form 5434-a - Application For Renewal Of Enrollment - Joint Board For The Enrollment Of Actuaries - 2017
Financial
 Form 5434-a - Application For Renewal Of Enrollment - Joint Board For The Enrollment Of Actuaries - 2012
Financial
Form 5434-a - Application For Renewal Of Enrollment - Joint Board For The Enrollment Of Actuaries - 2012
Financial
 Or Savings Incentive Match Plan For Employees Of Small Employers (simple Ira Plan)") Form 5306-a - Application For Approval Of Prototype Simplified Employee Pension (sep) Or Savings Incentive Match Plan For Employees Of Small Employers (simple Ira Plan)
Financial
Form 5306-a - Application For Approval Of Prototype Simplified Employee Pension (sep) Or Savings Incentive Match Plan For Employees Of Small Employers (simple Ira Plan)
Financial
 Or Savings Incentive Match Plan For Employees Of Small Employers (simple Ira Plan)") Form 5306-a - Application For Approval Of Prototype Simplified Employee Pension (sep) Or Savings Incentive Match Plan For Employees Of Small Employers (simple Ira Plan)
Financial
Form 5306-a - Application For Approval Of Prototype Simplified Employee Pension (sep) Or Savings Incentive Match Plan For Employees Of Small Employers (simple Ira Plan)
Financial
 Or Savings Incentive Match Plan For Employees Of Small Employers (simple Ira Plan)") Form 5306-a - Application For Approval Of Prototype Simplified Employee Pension (sep) Or Savings Incentive Match Plan For Employees Of Small Employers (simple Ira Plan)
Financial
Form 5306-a - Application For Approval Of Prototype Simplified Employee Pension (sep) Or Savings Incentive Match Plan For Employees Of Small Employers (simple Ira Plan)
Financial
 Or Savings Incentive Match Plan For Employees Of Small Employers (simple Ira Plan)") Form 5306-a - Application For Approval Of Prototype Simplified Employee Pension (sep) Or Savings Incentive Match Plan For Employees Of Small Employers (simple Ira Plan)
Financial
Form 5306-a - Application For Approval Of Prototype Simplified Employee Pension (sep) Or Savings Incentive Match Plan For Employees Of Small Employers (simple Ira Plan)
Financial


Related Categories
Parent category: Business