Consent Form Hiv Test Page 29
ADVERTISEMENT
 1
1 2
2 3
3 4
4 5
5 6
6 7
7 8
8 9
9 10
10 11
11 12
12 13
13 14
14 15
15 16
16 17
17 18
18 19
19 20
20 21
21 22
22 23
23 24
24 25
25 26
26 27
27 28
28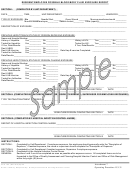 29
29 30
30 31
31 32
32 33
33 34
34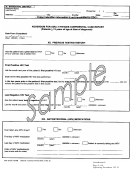 35
35 36
36 37
37 38
38 39
39 40
40 41
41 42
42RESIDENT/EMPLOYEE POSSIBLE BLOOD/BODY FLUID EXPOSURE REPORT
SECTION I:
(COMPLETED BY UNIT/DEPARTMENT)
DATE:_____________ TIME:_________ UNIT/DEPARTMENT: ___________________________________ WARD/POD:_______
TYPE OF EXPOSURE: Bite _________ Needle Stick _________ Open Wound _________ Mucous membrane/mouth _________
Mucous membrane/eyes_________ Sexual contact_________ Other (specify)_______________________
DESCRIPTION OF EXPOSURE: _______________________________________________________________________________
_______________________________________________________________________________
PREVIOUS HEPATITIS/HIV STATUS OF PERSON RECEIVING EXPOSURE:
Name and Hospital Number: ___________________________________________________________________________________
History of Hepatitis:
Yes __________ No __________
History of HIV:
Yes __________ No __________
Tested for Hepatitis:
Yes __________ No __________
Tested for HIV:
Yes __________ No __________
If Yes, Date/Results:
____________________________
If Yes, Date/Results: ____________________________
Rec’d HBIG:
Yes __________ No __________
Rec’d HB Vaccine:
Yes __________ No __________
Date Hep B vaccine Completed: ____________________
Tested for Antibodies:
Yes __________ No __________
Date/Results:_____________________________________
PREVIOUS HEPATITIS/HIV STATUS OF PERSON CAUSING EXPOSURE:
Name and Hospital Number: ___________________________________________________________________________________
History of Hepatitis:
Yes __________ No __________
History of HIV:
Yes __________ No __________
Tested for Hepatitis:
Yes __________ No __________
Tested for HIV:
Yes __________ No __________
If Yes, Date/Results:
____________________________
If Yes, Date/Results: ____________________________
Rec’d HBIG:
Yes __________ No __________
Rec’d HB Vaccine:
Yes __________ No __________
Date Hep B vaccine Completed: ____________________
Tested for Antibodies:
Yes __________ No __________
Date/Results:_____________________________________
___________________________________________
_________________
SIGNATURE/PERSON COMPLETING SECTION I
DATE
*******************************************************************************************************************
SECTION II: (COMPLETED BY UNIT/DEPARTMENT FOR RESIDENT EXPOSURE; SUPERVISOR FOR EMPLOYEE EXPOSURES)
TYPE TESTING/TREATMENT ORDERED ________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________
_________________
SIGNATURE/PERSON COMPLETING SECTION II
DATE
*******************************************************************************************************************
SECTION III: (COMPLETED BY HOSPITAL INFECTION CONTROL NURSE)
REPORT OF HOSPITAL INFECTION CONTROL NURSE ____________________________________________________________
___________________________________________________________________________________________________________
___________________________________________
_________________
SIGNATURE/PERSON COMPLETING SECTION III
DATE
INSTRUCTIONS:
SECTION I:
Completed by Unit/Department. If employee exposure, the employee should personally write the “Description of
Exposure,” if resident exposure, the nurse or supervisor should complete the “Description of Exposure.”
SECTION II:
Completed by Unit Department if resident exposure; Supervisor if employee exposure.
SECTION III:
Completed by the Hospital Infection Control Nurse.
GENERAL:
Sections I and II are to be completed as soon as possible after exposure occurs. All completed forms are to be
forwarded to the Office of Quality Assessment and Planning/Hospital Infection Control and Office of Risk Management
within forty-eight (48) hours.
Form 180, (Revised) Apr 09
Attachment 7
Office of Primary Responsibility
: Quality Assessment & Planning/Infection Control
Operating Procedure 153-31
ADVERTISEMENT
0 votes
Related Articles
Related forms
 Antibody Test Consent Form (rapid Testing)")









Related Categories
Parent category: Legal