Dd Form 2656 Instructions - Data For Payment Of Retired Personnel - April 2009 Page 3
ADVERTISEMENT
 1
1 2
2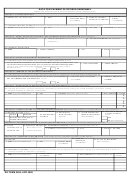 3
3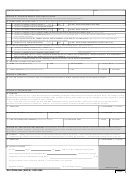 4
4DATA FOR PAYMENT OF RETIRED PERSONNEL
(Please read Instructions and Privacy Act Statement before completing form.)
SECTION I - PAY IDENTIFICATION
5. DATE OF
3. RETIREMENT/
1. NAME
2. SSN
4. RANK/PAY GRADE/
(LAST, First, Middle Initial)
TRANSFER DATE
BIRTH
BRANCH OF SERVICE
(YYYYMMDD)
(YYYYMMDD)
6. CORRESPONDENCE ADDRESS
(Ensure DFAS - Cleveland Center is advised whenever your correspondence address changes.)
a. STREET (Include apartment number)
b. CITY
c. STATE d. ZIP CODE
e. TELEPHONE (Incl. area code)
SECTION II - DIRECT DEPOSIT/ELECTRONIC FUND TRANSFER (DD/EFT) INFORMATION (See Instructions)
7. ROUTING NUMBER
8. TYPE OF ACCOUNT
9. ACCOUNT NUMBER
(See Instructions)
(Savings (S) or
(See Instructions)
Checking (C))
10. FINANCIAL INSTITUTION
a. NAME
b. STREET ADDRESS
c. CITY
d. STATE e. ZIP CODE
SECTION III - SEPARATION PAYMENT INFORMATION
11. Complete if you have received any one of the payment types listed in 11.a.
a. DID YOU RECEIVE SEVERANCE PAY (SE), READJUSTMENT PAY (RP), SEPARATION PAY (SP),
b. TYPE OF PAYMENT
c. GROSS AMOUNT
VOLUNTARY SEPARATION INCENTIVE (VSI), OR SPECIAL SEPARATION BONUS (SSB)?
(X one. If "Yes," attach a copy of the orders which authorized the payment, and a copy of
the DD Form 214.)
YES
NO
SECTION IV - MEMBER OF THE RESERVE COMPONENT
12. Complete only if a member or former member of the reserve component not on active duty retiring at age 60.
a. DO YOU RECEIVE OR WERE YOU RECEIVING ON THE DATE OF RETIREMENT
b. EFFECTIVE DATE OF PAYMENT
c. MONTHLY AMOUNT OF
ANY VA COMPENSATION FOR DISABILITY? (X one)
(YYYYMMDD)
PAYMENT
YES
NO
SECTION V - DESIGNATION OF BENEFICIARIES FOR UNPAID RETIRED PAY (See INSTRUCTIONS)
13. Complete this section if you wish to designate a beneficiary or beneficiaries to receive any unpaid retired pay you are due at death.
(Continue in Section X, "Remarks," if necessary.)
a. NAME (Last, First, Middle Initial)
b. SSN
c. ADDRESS (Street, City, State, ZIP Code)
d. RELATIONSHIP e. SHARE
%
%
%
%
%
SECTION VI - FEDERAL INCOME TAX WITHHOLDING INFORMATION
(Submit information in Items 14 - 17 in lieu of IRS Form W-4 for tax purposes.)
18. ARE YOU A UNITED
15. TOTAL NUMBER
16. ADDITIONAL
17. I CLAIM EXEMPTION
14. MARITAL STATUS
(X one)
STATES CITIZEN?
OF EXEMPTIONS
WITHHOLDING
FROM WITHHOLDING
SINGLE
MARRIED
(X one)
CLAIMED
(Optional)
(Enter "EXEMPT")
YES
MARRIED BUT WITHHOLD AT
HIGHER SINGLE RATE
NO (See Instructions)
SECTION VII - VOLUNTARY STATE TAX WITHHOLDING INFORMATION (Complete only if monthly withholding is desired.)
19. STATE
20. MONTHLY AMOUNT
21. RESIDENCE ADDRESS
(If different from address listed in Item 6)
DESIGNATED TO
(Whole dollar amount
a. STREET (Include apartment number)
b. CITY
c. STATE d. ZIP CODE
RECEIVE TAX
not less than $10.00)
SECTION VIII - DEPENDENCY INFORMATION (This section must be completed regardless of SBP Election.)
23. DATE OF
24. PLACE OF MARRIAGE
22. SPOUSE
MARRIAGE
c. DATE OF BIRTH
(See Instructions)
a. NAME (Last, First, Middle Initial)
b. SSN
(YYYYMMDD)
(YYYYMMDD)
25. DEPENDENT CHILDREN (Indicate which child(ren) resulted from marriage to former spouse by entering (FS) after relationship in column d.
Continue in Section X, "Remarks," if necessary.)
b. DATE OF BIRTH
e. DISABLED?
d. RELATIONSHIP (Son, daughter,stepson, etc.)
a. NAME (Last, First, Middle Initial)
c. SSN
(YYYYMMDD)
(Yes/No)
DD FORM 2656, APR 2009
ADVERTISEMENT
0 votes
Related Articles
Related forms
 Termination Request - April 2009")




")




Related Categories
Parent category: Business