Assessment Form
ADVERTISEMENT
 1
1 2
2 3
3 4
4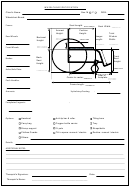 5
5PATIENT NAME___________________________
PATIENT ID # ____________________________
ASSESSMENT FORM
Name:
Sex: M
F
DOB:
Address:
Phone No.:
Therapist:
Agency:
Wheelchair being considered: Manual
Elec.
Assessment Date:
People consulted:
MEDICAL HISTORY
Diagnosis/Onset:
Stable
Detoriating
Past Surgeries:
Bone
Skin
Muscle
Other
Orthotics/Prosthetics:
Medications:
Medical Doctor:
Ph:
Health Professional(s):
Ph:
SOCIAL HISTORY
Lives alone
Spouse
Other Family
Friend
Other
Primary Carer details: (eg general health, agency contact)
Home/Unit
Retirement Village
Condo
Other
Accomodation:
Ownership: Owner
Rents
Other
: (note accessibility, etc.)
Primary Living/Work Environment
Narrowest Doorway:
Type of setting:
Rural
Suburban
Urban
Sidewalks
Paved Roads
Rough Terrain
Other locations where w/c will be used:
Intends to use at night:
Yes
No
Transportation :
Car (passenger)
Car (driver)
Van
Bus
Taxi
Other
Details:
FUNCTIONAL STATUS
Transfers:
Hoist
Standing pivot
Non-standing pivot
Pull to stand
Push to stand
Sliding
Other:
Details/Assistance:
Observed:
Yes
No
Ambulation status: (note device used)
Wheelchair Use: Independent
Assisted
Dependent
Hours/Day:
ADVERTISEMENT
0 votes
Related Articles
Related forms









")
Related Categories
Parent category: Medical