Assessment Form Page 4
ADVERTISEMENT
 1
1 2
2 3
3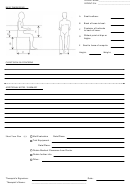 4
4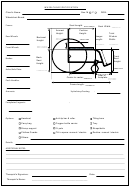 5
5PATIENT NAME___________________________
PATIENT ID # ____________________________
BASIC DIMENSIONS
Seat to elbow:
A
Back of knee to heel:
B
Posterior of buttocks
C
to back of knee:
Widest point at hips or
D
thighs:
Seat to base of scapula:
E
Height:
Weight:
CLIENT GOALS & CONCERNS
ADDITIONAL NOTES / SUMMARY
Mat Evaluation
Date/Place:
Short Term Plan
(s ):
Trial Equipment :
Date/Place:
Obtain Medical Clearance from Doctor
Obtain further info.
Other:
Therapist’s Signature:
Date:
Therapist’s Name:
__________________________________________
ADVERTISEMENT
0 votes
Related Articles
Related forms









")
Related Categories
Parent category: Medical