Assessment Form Page 5
ADVERTISEMENT
 1
1 2
2 3
3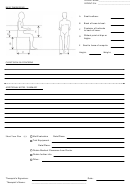 4
4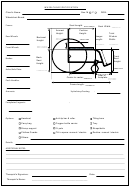 5
5WHEELCHAIR SPECIFICATION
Client’s Name:
Sex: M
F
DOB:
Wheelchair Brand:
Frame:
Seat Length:
Seat Width:
Armrest
Cushion
Height:
Height:
Total
W/chair
Hanger
Rear Wheels:
Backrest
Width:
Length:
Height:
Front Wheels:
Front
Back
Brakes:
Seat
Seat
Height:
Height:
Axles/Axle Plate:
Seat to
Castor to castor:
footplate:
Push Handles:
Frame length:
:
Armrests:
Upholstery/Seating
Footplates/Legrests:
:
Headrest
Anti-tip bar & roller
Tilting bars
Options:
Carry bag
Oxygen bottle carrier
Tray
Stump support
IV pole
Straps/belts
Clothes Guards
Tilt in space: manual / electric
Recline: manual / electric
Others:
Details:
ADDITIONAL NOTES:
Therapist’s Signature:
Date:
Therapist’s Name:
___________________________________________
ADVERTISEMENT
0 votes
Related Articles
Related forms









")
Related Categories
Parent category: Medical