Assessment Form Page 3
ADVERTISEMENT
 1
1 2
2 3
3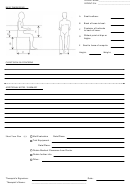 4
4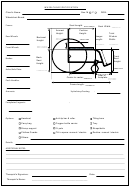 5
5PATIENT NAME___________________________
PATIENT ID # ____________________________
CURRENT SEATED POSITION
(as best evaluated – note fixed positions)
Balance/Trunk Control:
Rotated:
R
L
Neutral
Hyperextended
Fwd flexed
R
L
Laterally flexed:
Head:
L
Level
Elevated:
R
L
Sublaxed:
R
L
Shoulders:
Neutral
Elevated:
R
L
Rotated fwd:
R
L
Rib Cage:
Neutral
Scoliosis, apex on :
R
L
Kyphosis:
Spine:
Normal lumbar space
Flat Lumbar Space
Hyper-lordotic
Neutral
Posterior Tilt
Anterior Tilt
Rotated fwd:
R
L
Pelvis:
Oblique, lower:
R
L
Other:
Extended:
R
L
Abducted:
R
L
Adducted:
R
L
Flexed:
R
L
Hips:
Flexed (beyond 90º):
R
L
Extended (beyond 90º):
R
L
Knees:
Dorsiflexed:
R
L
Plantarflexed:
R
L
Supinate/Inv:
R
L
Feet:
Pronate/Evert:
R
L
Other:
Spasticity/ Reflexes/Tone:
Comments:
WHEELCHAIR HISTORY
Manual
Elec.
Model:
Period of use:
1.
Folding
Rigid
Armrest Hgt:
Hanger length:
Frame
Depth:
Width:
Hgt (front):
Hgt (back):
Seat
Other measurements:
Accessories/Features:
Issues:
Hx of accidents/collisions:
Manual
Elec.
Model:
Period of use:
2.
Folding
Rigid
Armrest Hgt:
Hanger length:
Frame
Depth:
Width:
Hgt (front):
Hgt (back):
Seat
Other measurements:
Accessories/Features:
Issues:
Hx of accidents/collisions:
ADVERTISEMENT
0 votes
Related Articles
Related forms









")
Related Categories
Parent category: Medical