Instructions For Filing: Personal & School District Income Tax - Department Of Taxation State Of Ohio - 2014 Page 28
ADVERTISEMENT
 1
1 2
2 3
3 4
4 5
5 6
6 7
7 8
8 9
9 10
10 11
11 12
12 13
13 14
14 15
15 16
16 17
17 18
18 19
19 20
20 21
21 22
22 23
23 24
24 25
25 26
26 27
27 28
28 29
29 30
30 31
31 32
32 33
33 34
34 35
35 36
36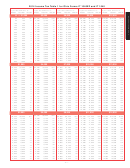 37
37 38
38 39
39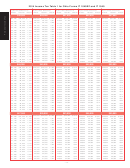 40
40 41
41 42
42 43
43 44
44 45
45 46
46 47
47 48
48 49
49 50
50 51
51 52
52 53
53 54
54 55
55 56
56 57
57 58
58 59
59 60
602014 Ohio Forms IT 1040EZ / IT 1040 / Instructions
Example 1: Sue has a health care insurance
your spouse were eligible to participate in a
plan. Sue cannot use her $50 monthly pay-
Medicare and/or a subsidized health insur-
plan through her employer. The health care
ment on line 2a of the worksheet, but she
insurance premium for this coverage is $265
ance plan.
can include this amount on Line 2.
every two weeks, of which $100 is deducted
Note: You must reduce the unsubsidized
Example 2: Sue is retired and qualifi es for
from Sue’s post-tax pay and $165 is paid by
medical care insurance premium amount
Medicare for the entire year. She pays $50
her employer. The taxpayer can include on
you enter on line 2a of the worksheet by the
each month for unsubsidized supplemental
line 2 of the worksheet the $100 insurance
amount of the self-employed health insur-
health insurance and $20 each month for
premiums that she paid.
ance deduction that you claimed on line 29
Medicare B premiums. Sue can include her
of federal form 1040.
$50 monthly premium payments on line
Line 2a – Unsubsidized Medical Care
Insurance Premiums
2a of the worksheet as she is eligible for a
Example 1: Sue has a health care insur-
If you were eligible to participate in a sub-
subsidized plan through Medicare; Also, she
ance plan through her employer. She has
sidized health care plan, enter on line 2a of
can include the $20 Medicare B premium
$50 deducted from her paycheck (post-tax)
the worksheet the costs for unsubsidized
payments amounts on line 2.
each month to pay for her portion of her
medical care insurance premiums you paid
health care insurance premium costs. Her
Note: If you are eligible for Medicare cover-
for dental, vision and health insurance for
employer contributes $450 each month
age, you can use line 2a of the worksheet
you, your spouse and dependents. If you or
toward the health care insurance premium
to report any unsubsidized medical care
your spouse were eligible to participate in
costs that total $500 each month. This is a
insurance premiums paid while you were
a subsidized plan for part of the year, enter
subsidized plan, so Sue is not participating
eligible for Medicare coverage.
on this line the unsubsidized premiums for
in an unsubsidized health care insurance
the portion of the year during which you or
Unreimbursed Health Care Expenses Worksheet for Line 46a
Do not include on this worksheet any amounts excluded from federal adjusted
gross income under a cafeteria plan (see Internal Revenue Code 125) or under any fl exible spending account.
1. Were you eligible to participate in any subsidized health insurance plan / Medicare for (check one of the following):
A. The entire year;
B. None of the year; OR
C. Part of the year (see Note 1, below)
2. Enter the medical care expenses you paid and any subsidized medical insurance premiums you
paid for dental, vision and health insurance. Ohio Revised Code (R.C.) 5747.01(A)(11)(b)
.................... 2.
2a. Enter the amount you paid for unsubsidized medical care insurance premiums for dental, vision and
health insurance. R.C. 5747.01(A)(11)(b)
If you checked A on line 1, enter your unsubsidized premiums on this line.
If you checked B on line 1, enter -0-.
If you checked C on line 1, enter your unsubsidized premiums for the part of the year in which you
were eligible to participate in a subsidized health insurance plan or Medicare.
................................. 2a.
..................................................................................................................................... 3.
3. Add lines 2 and 2a
..... 4.
4. Enter your federal adjusted gross income (from line 1 of Ohio form IT 1040). If less than -0-, enter -0-
5. Multiply line 4 times the statutory factor of 7.5%
....................................................................................... 5.
6. Line 3 minus line 5. If less than -0-, enter -0-
............................................................................................ 6.
7. Enter the amount for unsubsidized premiums you paid for long-term care insurance (see Note 2,
below). R.C. 5747.01(A)(11)(a)
................................................................................................................ 7.
8. Enter the amount you paid for unsubsidized medical care insurance premiums, including those for
dental, vision and health insurance. R.C. 5747.01(A)(11)(a)
If you checked A on line 1, enter -0-.
If you checked B on line 1, enter your unsubsidized premiums on this line
If you checked C on line 1, enter this amount for the part of the year that you were not eligible to
participate in a subsidized health insurance plan or Medicare.
............................................................ 8.
9. Enter the amount paid by your employer and included in your federal adjusted gross income solely
because it relates to an "accident and health plan" for qualifying relatives and any amounts included in
your federal adjusted gross income that were paid through an employer-subsidized accident and health
plan to reimburse you for medical care expenses for qualifying relatives (see instructions for line 9). R.C.
5747.01(A)(11)(c)
....................................................................................................................................... 9.
10. Add lines 6, 7, 8 and 9. Enter the total on line 46a of Schedule A
........................................................... 10.
Note 1: If you or your spouse were eligible to participate in a subsidized plan for part of the year, check C on line 1 above and enter on line 2a these unsubsidized premiums
for the portion of the year during which you or your spouse were eligible to participate in a Medicare and/or a subsidized health insurance plan. Enter on line 8 any portion
of the unsubsidized premiums paid for dental, vision and health insurance for the portion of the year during which you or your spouse were not eligible to participate in a
Medicare and/or a subsidized health insurance plan (see instructions, Example 3).
Note 2: Do not enter any amounts on line 7 that are included on line 2, 2a, 8 or 9.
- 28 -
ADVERTISEMENT
0 votes
Related Articles
Related forms
 Instructions For Filing: Personal & School District Income Tax & Telefile - Department Of Taxation State Of Ohio - 2012
Financial
Instructions For Filing: Personal & School District Income Tax & Telefile - Department Of Taxation State Of Ohio - 2012
Financial
 Instructions For Filing The School District Estate Income Tax Return - Ohio School District Income Tax
Financial
Instructions For Filing The School District Estate Income Tax Return - Ohio School District Income Tax
Financial



 Instructions For Form It-2210 - Interest Penalty On Underpayment Of Ohio Or School District Income Tax
Financial
Instructions For Form It-2210 - Interest Penalty On Underpayment Of Ohio Or School District Income Tax
Financial
 Instructions For Form It-2105 - Estimated Income Tax Payment Voucher For Individuals - New York State Department Of Taxation And Finance - 1999
Financial
Instructions For Form It-2105 - Estimated Income Tax Payment Voucher For Individuals - New York State Department Of Taxation And Finance - 1999
Financial
 Instructions For Form It-220 - Minimum Income Tax - New York State Department Of Taxation And Finance - 2004
Financial
Instructions For Form It-220 - Minimum Income Tax - New York State Department Of Taxation And Finance - 2004
Financial


Related Categories
Parent category: Financial