Form Rv-2 - All-Terrain Vehicle Dealer Registration Instructions Page 20
ADVERTISEMENT
 1
1 2
2 3
3 4
4 5
5 6
6 7
7 8
8 9
9 10
10 11
11 12
12 13
13 14
14 15
15 16
16 17
17 18
18 19
19 20
20 21
21 22
22 23
23 24
24 25
25 26
26 27
27 28
28 29
29 30
30 31
31 32
32 33
33 34
34 35
35 36
36 37
37 38
38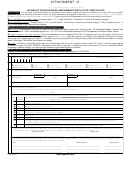 39
39 40
40 41
41 42
42 43
43 44
44 45
45 46
46 47
47 48
48 49
49 50
50 51
51 52
52 53
53 54
54 55
55 56
56ATTACHMENT A
New York State Department of Motor Vehicles
ORIGINAL FACILITY APPLICATION
Investigation Required
Facility No. ____________________________
Facility Type and Control No.
Appr/Denied
Expiration Date ________________________
1-A
E
RS
RSB
DIA
Current Header Exp. Date ________________
1-B
C
ISP
ISD
ISF
Cross Ref. Old Fac. __________________
2-A
M
DLQ
DLN
DLU
Add OOB __________________________
2-B Bonding DLW
DLB
DLS
Remove OOB
3
A
TRS
DIS
SLP
Amend Head Exp. From ______ To ______
D
B
IVC
MCC
SCP
Amend Facility Type From _____ To______
I
C
PSP
907
Orig w/exist Record
Add Business
E
Analyzer Ident. No. ______________________
DL
Total Fee
SCC
YTB
DO NOT WRITE IN THE SHADED AREAS OF THIS APPLICATION.
FOLLOW THE INSTRUCTIONS ON FORM VS-1.1 TO COMPLETE THIS APPLICATION CORRECTLY.
BE SURE TO COMPLETELY ANSWER ALL OF THE QUESTIONS ON PAGES 1 AND 2 OF THIS APPLICATION, AND ALL OF THE
QUESTIONS IN WHICHEVER SECTION(S) ON PAGES 3 AND 4 PERTAIN TO YOUR APPLICATION. WE CANNOT PROCESS
INCOMPLETE APPLICATIONS.
1. Your Facility Name (DBA Name)
Facility Name
Three of Name
Name Overflow
2. Your Facility Address - Number and Street
3. Facility Phone No.
(
)
Street
4. Your Facility Address - City
State
Zip Code
County
City/State
ZIP/County
5. Type of Ownership
Individual
Partnership
Corporation
Governmental
Educational
Franchise
Chain
DBA
6. Owner/Corporation Name
Owner/Corp. Name
Name Overflow
7. Owner/Corporation Address - Number and Street
8. Owner/Corporation Phone No.
(
)
Street
9. Owner/Corporation Address - City
State
Zip Code
County
City/State
ZIP/County
VS-1 (6/06)
PAGE 1 OF 4
ADVERTISEMENT
0 votes
Related Articles
Related forms

 Form Rv-2 - Rental Motor Vehicle And Tour Vehicle Surcharge Tax Return Instructions - 2007
Financial
Form Rv-2 - Rental Motor Vehicle And Tour Vehicle Surcharge Tax Return Instructions - 2007
Financial
 Form Rv-2 - Rental Motor Vehicle, Tour Vehicle, And Car-sharing Vehicle Surcharge Tax - 2016
Financial
Form Rv-2 - Rental Motor Vehicle, Tour Vehicle, And Car-sharing Vehicle Surcharge Tax - 2016
Financial


")

")


Related Categories
Parent category: Legal